Authors’ note: CAP uses “Black” and “African American” interchangeably throughout many of our products. We chose to capitalize “Black” in order to reflect that we are discussing a group of people and to be consistent with the capitalization of “African American.” In this report, the terms “Black,” “African American,” “white,” and “other” do not include individuals who identify as Hispanic or Latinx, although we recognize that individuals who identify as Hispanic can be of any race. The group “non-Hispanic other” includes children identified as American Indian and Alaska Native; Native Hawaiian or other Pacific Islander; other race; and two or more races—all groups with sample sizes too small to yield reliable estimates.
Introduction and summary
Since the World Health Organization declared the COVID-19 outbreak a pandemic on March 11, 2020,1 the United States has seen a proliferation of cases, record-breaking unemployment, and economic instability.2 Meanwhile, many public health measures that severely restrict social interactions—including stay-at-home orders and school and child care closures, among others—have been prematurely lifted, with disastrous effects.3 And as news spread about the disproportionate impact of the pandemic on communities of color, high-profile acts of police violence against Black Americans helped reignite the Black Lives Matter movement.4 These events are profoundly transforming the lives of American adults. So how will children fare in the face of these rapid changes?
These recent events help illuminate the three Es of trauma: event, experience, and effects.5 In the case of the COVID-19 pandemic, the event—the threat of falling sick, economic uncertainty, and the disruption of relationships—is, in theory, shared nearly universally. However, an individual child’s experience is shaped by several factors, including financial and social resources, and mediated by their interactions with adults. A child’s specific experience helps determine whether the event will have negative effects on their well-being.6 Recent surveys of families’ experiences during the pandemic suggest parents affected by financial hardship are also experiencing greater distress, which in turn creates emotional difficulties among children.7 Adults in communities that for generations have been socially or economically marginalized by unjust policies may struggle to marshal enough financial and emotional resources to blunt the experience of stressful events. Indeed, research also suggests that even middle- and high-income Black and Latinx families are experiencing greater financial hardship as a result of the pandemic than other comparable households, giving researchers and policymakers reason to worry that the pandemic will widen existing inequalities in parent and child well-being.8
The pandemic and its economic and social fallout may have adverse effects in the lives of young children today, but these events are not unique. In the past 25 years, researchers, policymakers, and practitioners have focused on a subset of adverse events occurring in childhood, known as adverse childhood experiences (ACEs).9 These events are strongly associated with negative effects on a child’s physical, emotional, and social well-being throughout their life span.10 Little is known about the prevalence of adverse events during the developmentally sensitive early childhood period or how systemic inequities give rise to them early in life; however, it is known that their effects can last a lifetime.
This report provides new data on the prevalence of adverse events among children from birth through age 3. It concludes with policy recommendations for preventing, identifying, and mitigating the harmful effects of adversity, with an eye toward achieving racial and economic justice. Key findings from the analysis include:
- Most (71 percent) children ages 3 and younger have experienced no ACEs, 20 percent have experienced one ACE, and 8 percent have experienced two or more ACEs.
- Economic hardship is the most common form of adversity; about 1 in 5 young children live in a family that has struggled to cover basic needs such as food or housing.
- Even at this early age, there are wide racial disparities in exposure to adversity. Compared with young white children—of whom 7 percent experience multiple adversities—the percentage of children experiencing multiple adversities is approximately twice as high for Black and non-Hispanic other children, at 15 percent and 14 percent, respectively.
- Racial and ethnic disparities are found across several forms of adversity: economic hardship; parents’ divorce or separation; living with someone experiencing mental illness or severe depression; parental incarceration; and experiencing bias or discrimination.
Policymakers should implement policies that reduce the prevalence of adverse events and mitigate their negative effects and develop resources for practitioners and communities to effectively embed adversity screening within a broader system of culturally informed support. Understanding the roots of adversity in unjust systems is crucial throughout this process.
Background
Children’s brains form 1 million new neural connections every second in the first years of life.11 Genes provide a blueprint for how, when, and where neural connections form, but a child’s social environment helps determine which connections are built or strengthened over time.12 Adversity—including poverty, discrimination, and related environmental stressors—can affect the formation of important brain circuits.13 This is because prolonged or intense exposure to adversity in the absence of adequate support—a condition known as toxic stress—activates a child’s stress response past the point where it’s adaptive, leading to wear and tear on the developing brain and body.14 Although some adversity-induced developmental impacts can be repaired, especially through supportive relationships with adults,15 many of the impacts are long-lasting. Importantly, conditions such as poverty and community disinvestment that foment unmitigated, toxic stress in children are the product of white supremacist policies that have historically benefited white families to the detriment of families of color.16 Thus, children who experience toxic stress are at risk of not reaching their full potential,17 at least partly due to unjust societal values and policies.
The Centers for Disease Control and Prevention defines ACEs as a subset of potentially traumatic childhood events that may harm children’s sense of security, stability, and bonding with caregivers and others.18 These experiences may serve as useful markers for possible toxic stress.19 Individuals react differently to negative events, based on a variety of factors including material and social resources. Importantly, however, exposure to adverse events does not itself represent a health problem or diagnosis per se, just as living through the pandemic does not guarantee a child will develop trauma or poor health outcomes.
There is no single, comprehensive list of negative experiences that encompasses all ACEs. The original ACEs study in the 1990s asked a large sample of adults about seven childhood experiences, including psychological, physical, and sexual abuse, as well as exposure in the home to substance abuse, mental illness and suicide, incarceration, or violence.20 Since then, much research on ACEs has expanded to include physical and emotional neglect as well as measures of social marginalization that are designed to capture systematic prejudice and bias.21
In the original ACEs study and many others since, researchers have found strong associations between exposure to multiple forms of adversity—that is to say, having a higher ACEs study index, or total number of ACEs experienced prior to age 18—and poor physical and mental health outcomes in adulthood. These include heart disease and depression, and even early death.22 But negative adversity-induced outcomes can also manifest throughout childhood as learning and behavioral challenges and poor health.23 New evidence suggests that adversity and stress have intergenerational effects and can influence development in infancy and early childhood. Studies reveal that at as early as 18 months of age, children born to women who, through no fault of their own, had experienced multiple adversities in childhood, are more likely to exhibit negative emotional and physical health outcomes.24
Despite the increased attention to adverse events, there is relatively little research on their prevalence in early childhood,25 as most research on ACEs and other adverse events examines adults’ retrospective reports of their own experiences prior to age 18. Given the wealth of research on child development demonstrating that children’s brains are both most vulnerable and malleable in the early years,26 raising awareness about the prevalence of early adversity is critical. A better understanding of the prevalence of adversity and for specific demographic groups can inform research and policy actions to address some of the risks children face on the way to healthy development.27
Findings
CAP’s analysis uses a multiyear sample from 2016 to 2018 of the U.S. Census Bureau’s National Survey of Children’s Health (NSCH), a survey providing rich data on children’s physical and mental health as well as family and community characteristics. The NSCH, which relies on parent surveys, is the only survey of children’s health that includes a checklist of ACEs—also known as an ACEs index28—and is representative of all children younger than 18 years of age, both nationwide and within each state.29 Importantly, the NSCH does not survey families experiencing homelessness and thus likely undercounts severe forms of adversity that children disproportionately face in these circumstances. Moreover, children’s exposure to adversity is likely to increase in the wake of the pandemic, particularly for Black families and other families of color, who are most likely to experience the negative health and economic consequences of the coronavirus.30 (see the data and methodology detailed in the Appendix for additional information)
This analysis provides new data on the overall prevalence of adverse events as well as the types of challenges children from birth through age 3 experience—information essential to helping practitioners and policymakers prevent and mitigate the negative effects of adversity during the developmentally sensitive early childhood period.
Findings show that more than 1 in 4 children in the United States have been exposed to at least one adverse event, with children of color disproportionately more likely to experience adversity in early childhood.
More than 1 in 4 young children experience adversity
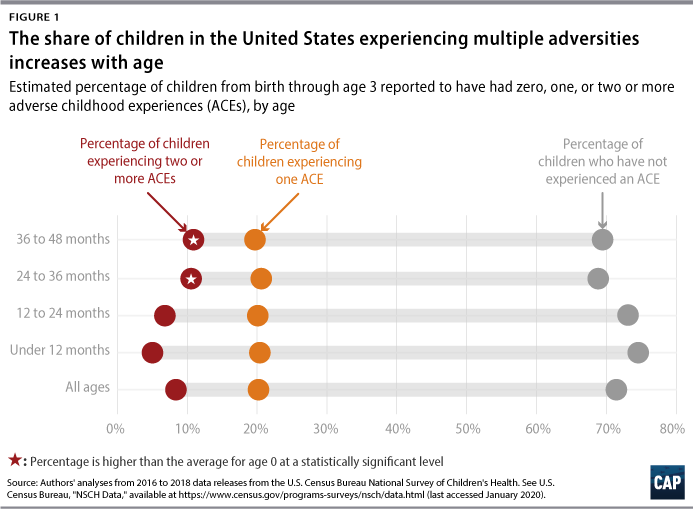
Figure 1 shows the distribution of the total number of adverse events, as reported by parents, for children from birth through age 3. Although most children in this age group had not experienced an ACE, 20 percent had experienced one ACE and 8 percent had experienced two or more ACEs.
As expected, the percentage of children experiencing multiple adversities increases with age, more than doubling between infants younger than 1 year old (5 percent) and children age 2 or older (11 percent).31 As exposure to four or more ACEs before age 18 is considered clinically significant; this means that even before entering preschool, more than 1 in 10 children are on a path that could make later school and economic success more difficult.
Economic difficulty is the most common form of adversity
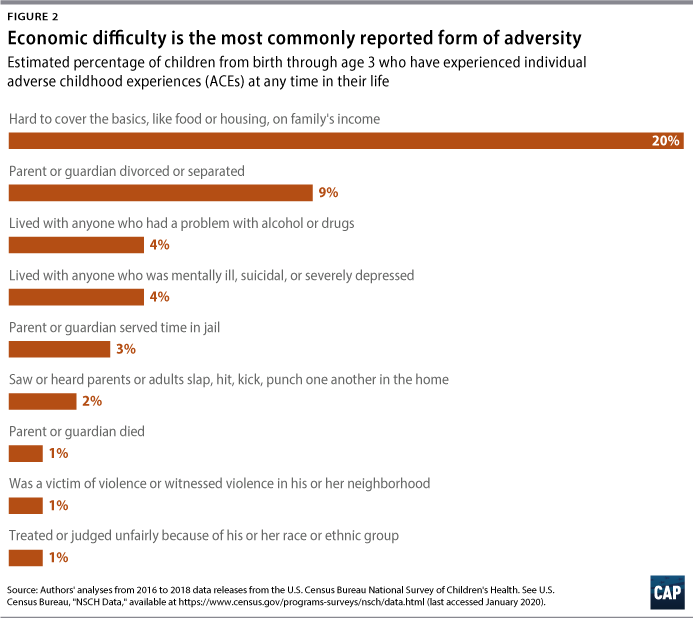
For infants and toddlers, economic hardship is the most common adversity or challenge; about 1 in 5 young children live in a family that has struggled to cover basics such as food or housing. This finding is consistent with earlier research demonstrating that families see their incomes drop while expenses and debt rise following the birth of a child.32 Parental divorce or separation is the second-most common hardship or adversity, with nearly 1 in 10 (9 percent) children experiencing this event prior to their 4th birthday. Other ACEs, such as parental incarceration or death, are rarer.
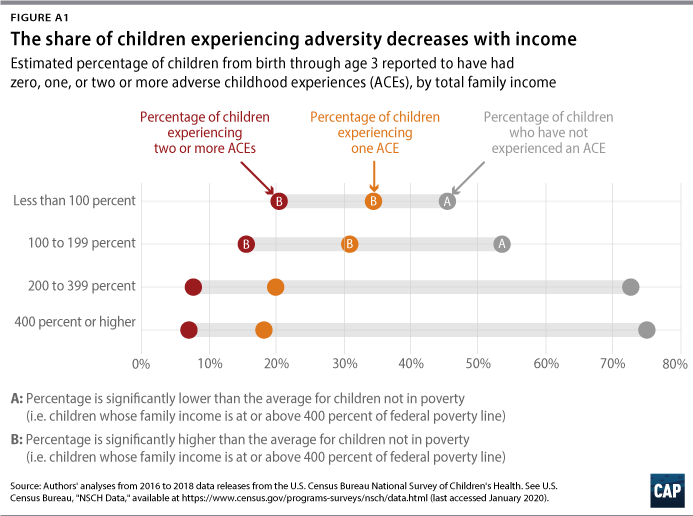
It should be noted that although economic hardship is the most common form of adversity, adversity finds children across the economic spectrum. Additional analyses reveal that the presence of multiple adversities decreases with family income; however, almost 7 percent of young children in families with incomes at least 400 percent above the federal poverty line have been exposed to two or more ACEs. (see the Appendix for additional information on individual ACEs)
Measurement of ACEs: Critical issues and limitations
Measuring childhood adversity is a difficult task because, as discussed by other researchers, no single questionnaire, form, or checklist used to screen for ACEs fully captures all forms of adversity.33 For example, experiences such as exposure to natural disasters, war or community violence, and forced displacement are often excluded. Other limitations and challenges of current ACEs measures include:
- Screening tools only capture exposure to adversity. Most ACEs screening tools consist of checklists tallying an individual’s exposure to an event and thus cannot capture their reactions, strengths, or broader contexts.34 In other words, screening tools fail to capture the experience or effects of adversity, instead focusing only on the event. ACEs screening tools can help identify children who may be at risk for toxic stress, trauma, or negative health consequences, although ACEs do not necessarily cause these harmful effects.35
- Screening tools lack cultural sensitivity or specificity. Although experiencing racism, bias, and discrimination is included in some current ACEs screening tools to identify social inequalities, many fail to capture how these and other events are embedded in a community’s history.36 Researchers should develop and use measures that capture symptoms of historical trauma, unique community strengths, and cultural understanding of adversity.37
- Screening tools weigh all adverse experiences equally. The severity, duration, or frequency of adverse events and how adults manage situations around the child matter to children’s development, but these characteristics are largely unmeasured in ACEs screening tools. For example, an ACEs score treats equally prolonged or severe physical abuse, frequent poverty spells, and a quickly resolved parental divorce that may ultimately leave both adults happier and healthier.38
- Limited research exists on the validity of screening tools in young children. Four ACEs before age 18 is considered clinically significant, but there is no analogous threshold for a “high” ACEs score or index in early childhood.39 Moreover, because young children are unable to report on exposure to adversity themselves, screening tools must be completed by an adult who may not complete the assessment or form accurately.40
- Screening tools make broad assumptions related to adults’ mental health. Currently, ACEs screening tools assume that the presence of a mental health disorder in a family member is an adverse experience for the children who live with them—an approach that yields imprecise results because it uses a diagnosis as a catchall for specific behaviors that affect a child’s development and home environment.41 In addition to being a blunt measure of adversity, this contributes to sanist perceptions of people with mental illness as inherently violent or unstable.
In sum, while the ACEs screen can provide useful information for targeting resources to communities in need, relying on a checklist of finite experiences to measure adversity—with little recognition for how adversity is understood or treated within communities—has its limitations.
Racial disparities in exposure to adversity arise in early childhood
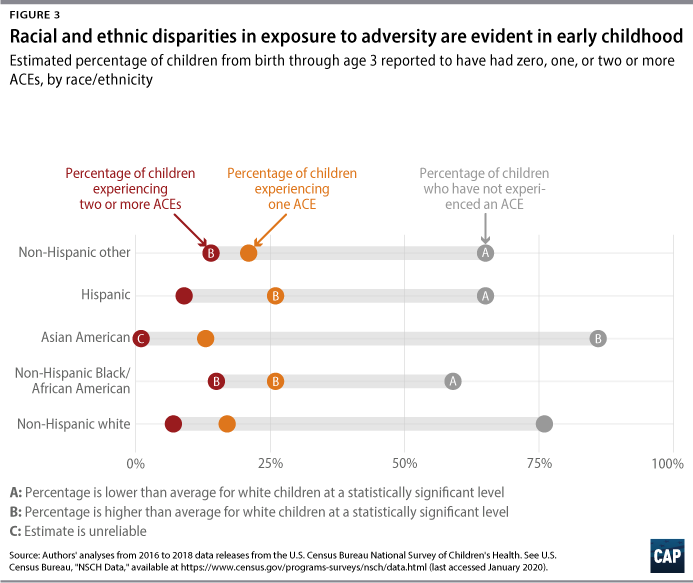
Figure 3 shows ACEs prevalence by children’s race and ethnicity and reveals that even at this early age, there are significant racial and ethnic inequalities in exposure to adversity. Compared with young white children, 7 percent of whom experience multiple adversities, the percentage is approximately twice as high for Black (15 percent) as well as non-Hispanic other children (14 percent), a diverse category including groups that are too small to be analyzed individually.42 The share of children exposed to one ACE is also significantly higher for Hispanic and Black children. Although previous research has shown inequalities in exposure to adversity throughout childhood, often stemming from structural and interpersonal racism, this analysis reveals just how early these disparities emerge.43
Children of color are more likely to experience most types of adversities
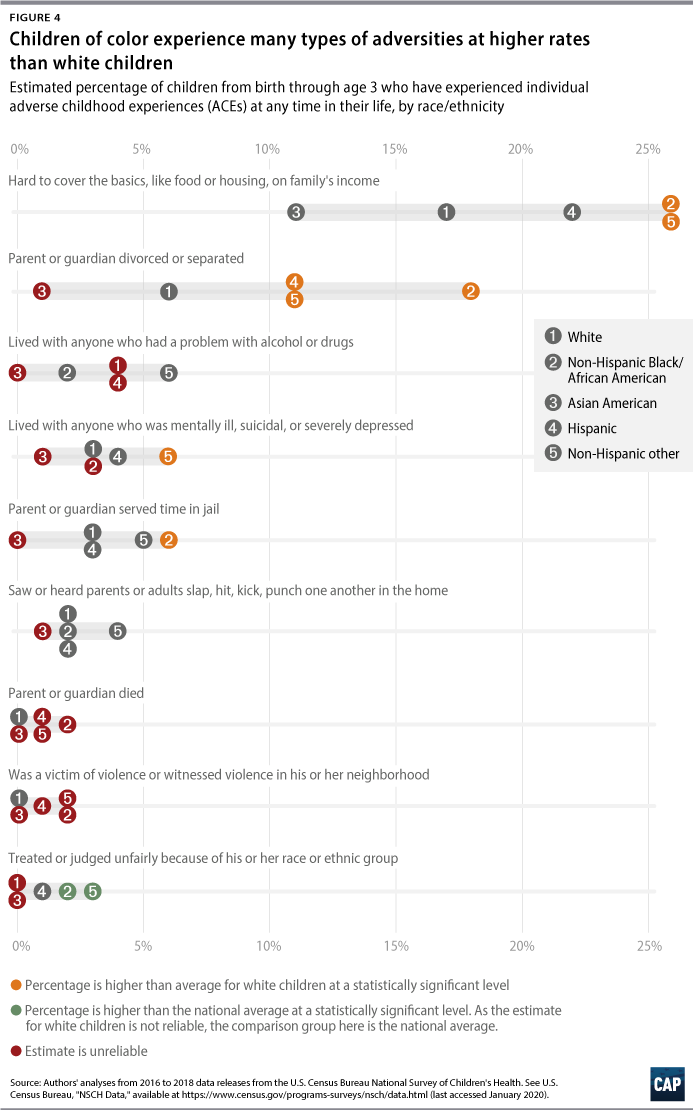
Figure 4 reveals that white children experience lower rates of most individual adversities than children from other racial and ethnic groups. Prevalence rates for individual forms of adversity for Asian American children are also low, but as these estimates are based on small sample sizes, they should be interpreted with caution.44 Moreover, the use of aggregate data on Asian American and Latinx children is extremely limited, as children in both of these groups have roots in dozens of diverse countries and represent a wide range of socioeconomic, linguistic, and cultural backgrounds.45
Like overall ACEs scores, substantial disparities across racial and ethnic groups in exposure to specific adversities are evident, with consistent and robust disparities among white, Black, and non-Hispanic other children. Compared with white children, Black children experience higher rates of economic hardship; parents’ divorce or separation; parental incarceration; and bias or discrimination.46 Non-Hispanic other children also experience higher rates of exposure to specific adversities, but the inherent diversity of this group makes interpreting this finding difficult and highlights the need for data collection that will support disaggregation by race. As factors such as occupational segregation and economic exploitation make families of color particularly vulnerable to economic downturns, disparities are likely to increase following the pandemic, as the economic impact of the coronavirus crisis will persist.47
Differences in exposure to adversity by race and ethnicity, especially when children are very young, reflect broader societal patterns of racial discrimination. For example, women of color earn less than white male counterparts in the same industries, a fact that undermines the economic stability of families of color with young children.48 Furthermore, these data show parental incarceration is twice as common among Black children as it is among white children, at 6 percent and 3 percent, respectively. However, the rest of the data reveal that equally small shares of both groups witness domestic violence or live with an adult who uses drugs or alcohol, strongly suggesting that bias in the criminal justice system, rather than differences in parents’ behavior, drives differences in parental incarceration. Evidence of racial bias in the criminal justice system burst into the news with recent high-profile police brutality cases, but it abounds in everything from sentencing length to treatment by police.49
Young children’s exposure to adversity varies across states
Table 1 shows the overall prevalence of adverse events by state, revealing geographic disparities among young children across the country. Compared with the national average, Massachusetts and Pennsylvania have significantly higher shares of children who have not experienced any adverse events, at 82 percent and 80 percent versus 71 percent, respectively, whereas Oklahoma and Arizona have significantly higher percentages of young children experiencing multiple adversities—21 percent and 15 percent versus 8 percent, respectively.
Although small sample sizes preclude analysis of what drives these geographic disparities, policies and societal choices at the state level—including decisions to address child poverty, support families, and address criminal justice inequities—can affect the overall prevalence of ACEs. For example, Oklahoma and Arizona have higher-than-average poverty rates for infants and toddlers and show room for improvement on an index of well-being developed by ZERO TO THREE and Child Trends. The opposite pattern is found in Massachusetts and Pennsylvania.50 Thus, state policy represents an opportunity to mitigate ACEs’ occurrence and negative effects.

States’ actions on addressing ACEs
As research on ACEs and trauma has grown, so has states’ interest in assessing and addressing childhood adversity. As of July 2020, the last date for which these data are available, 27 states have enacted legislation concerning ACEs,51 and at least 37 have or plan to have a statewide community-based collaborative initiative focusing on ACEs science, including trauma-informed resilience policy and practice.52 Although several states have enacted legislation to combat toxic stress, childhood trauma, or adversity,53 the following are a few examples of state policies and initiatives that address ACEs specifically.
Washington
Washington state passed a law in 2011 establishing a private-public initiative focused on identifying innovative strategies or activities to reduce and prevent ACEs, thereby becoming the first state to enact legislation regarding ACEs.54 A 2016 evaluation of these activities showed that they helped improve several targeted outcomes, including reductions in child abuse and neglect as well as improved school attendance.55
Vermont
In 2014, Vermont became the first state to propose a bill to integrate ACEs screening into health care settings. In addition to encouraging medical professionals to screen for ACEs, the bill also proposed integrating the science of adversity, trauma, and resilience into medical school curricula.56
California
Led by the efforts of Dr. Nadine Burke Harris—a pediatrician, ACEs researcher, and California’s first surgeon general—California is undertaking one of the most aggressive efforts to screen and address ACEs.57 Gov. Gavin Newsom (D) allotted $40.8 million in the 2019-2020 budget to the state’s Department of Health Care Services for screening for ACEs among children and adults enrolled in Medi-Cal, the state’s Medicaid program. Under this program, health providers can bill Medi-Cal for ACEs screening.58 It should be noted that although the 2020-2021 California state budget agreement passed in June 2020 continues funding for screening, it withdrew the $10 million budget request granted in January for a public awareness campaign and training program.59
Colorado
In July 2020, Gov. Jared Polis (D) signed into law a bipartisan bill to create a professional development plan for the early childhood workforce, support mental health consultants, and include training on ACEs, the science of resilience, and trauma-informed practices and interventions.60
Recommendations
Interest in early childhood adversity from the research, health care, and policy communities has grown tremendously in the decades since the original ACEs study publication.61 The analysis presented in this report shows that even young children face adversity that can fundamentally change their lives. The preponderance of early childhood adversity, particularly among children of color, reflects larger societal values about who deserves support; a society claiming to care about children must grapple with this reality and act accordingly. The current pandemic and economic crises—which are disproportionately harming Black families and other people of color62—are likely to expose many more young children to adverse events and deepen disparities, which makes preventing and mitigating their harm even more pressing. These findings should compel policymakers to take deliberate and effective action now and beyond the current crisis.
Policymakers should consider the following recommendations to address childhood adversity.
Implement and expand strategies that reduce the likelihood of early adversity
Policymakers should implement policies that reduce financial hardship, the most common form of adversity and an especially acute challenge for the families of newborns.63 Policies targeted for families with very young children—including paid family and medical leave and affordable child care for infants and toddlers—are key in the wake of the pandemic and beyond, as are those that reduce child poverty, such as providing adequate wages, nutrition and housing assistance, and a progressive tax policy.64 These policies, which have often excluded families of color, are particularly important for narrowing the racial inequalities that are sure to widen without aggressive action. Policies that clear criminal records also reduce intergenerational poverty by allowing individuals to reenter the workforce more easily.65 Other criminal justice reforms—including sentencing reform and evidence-based violence prevention programs—reduce children’s exposure to other adverse events, including parental incarceration and neighborhood violence.66
Increase the availability and accessibility of evidence-based services
Screening for adversity is only one component of a comprehensive, strengths-based approach to address childhood adversity.67 Expansions in infant mental health and early intervention services—for example, those outlined in the Individuals with Disabilities Education Act Part C—to serve children at risk may help reach children and families early who are coping with toxic stress or trauma. Evidence-based family support programs such as maternal and early childhood home visiting, which connect families with a nurse, social worker, or other skilled professional, can also help families to access community resources and further trauma-informed care. Federal policymakers should therefore substantially increase funding to programs such as early intervention and the Maternal, Infant, and Early Childhood Home Visiting Program as well as ensure adequate access to mental health services through publicly funded insurance.
Increased access to affordable, high-quality early care and education also provides intergenerational benefits, encouraging family self-sufficiency and promoting children’s health and development.68 With unemployment rates at record highs and child care growing even harder to find and afford, policymakers should substantially increase funding to the Child Care and Development Block Grant and Early Head Start/Head Start, the latter of which has launched a campaign to address childhood trauma.69
Support the development of better screening tools and practices
Researchers should partner with community-based groups to develop culturally and developmentally appropriate tools that capture adversity data in a way that reflects the breadth of challenges some children face while not inadvertently penalizing them.70 Policymakers should dedicate funding to this research and for training so that all individuals who conduct screenings can complete this sensitive process without retraumatizing both parents and children.71 Developmental and behavioral screenings are particularly important to identify children who may have experienced adverse events and to treat adversity-induced developmental challenges and trauma early and effectively.
Fund high-quality longitudinal research on adversity
To the authors’ knowledge, most research on ACEs—including this report—relies on cross-sectional data. As a result, researchers know little about how ACEs accumulate over an individual life span or how these patterns vary with race or ethnicity. Whether funding comes exclusively from federal or state governments, or a combination of public and private dollars, it must be robust and stable enough to support data collection over several years. This research should also support data that can be disaggregated by race, which may involve oversampling small groups—such as American Indian and Alaska Native, Native Hawaiian, Asian American, and Latinx people—and partnering with communities to conduct culturally appropriate research.72
Conclusion
Understanding the prevalence and types of adverse events during the developmentally sensitive early childhood period is a vital first step in mitigating their harm to children’s long-term health and academic and economic success. The ongoing COVID-19 pandemic, sure to touch so many young children, has the potential to exacerbate the adverse events in young children’s lives and introduce new ones, all while deepening shameful inequalities. Ultimately, however, policymakers should seek to do more than identify and prevent these adverse experiences; they must invest in strategies that expand economic and educational opportunity to ensure all young children have what they need to learn and grow, even during crises. The pandemic and recession make these investments even more important.
About the authors
Cristina Novoa is a former senior policy analyst for Early Childhood Policy at the Center for American Progress.
Taryn Morrissey is a senior fellow for Early Childhood Policy at the Center and an associate professor in the Department of Public Administration and Policy at American University.
Acknowledgements
The authors would like to thank the many reviewers of this report for their valuable feedback and partnership. In particular, they would like to thank Azza Altiraifi from the Disability Justice Initiative; Connor Maxwell, formerly of the Race and Ethnicity Policy team; Jaboa Lake and Rejane Frederick of the Poverty to Prosperity Program; Betsy Pearl of the Criminal Justice Reform team; Simon Workman and Katie Hamm of the Early Childhood Policy team; the Art and Editorial teams; and many others.
Appendix
Data and methodology
This report presents findings from CAP’s analysis of a combined multiyear sample of the U.S. Census Bureau’s National Survey of Children’s Health.73 The NSCH is the only survey on the health and well-being of children and families that is representative of all noninstitutionalized children ages 0 to 17, nationwide and within each state. Researchers contact households at random using an address-based sample to identify those with one or more children younger than 18 years old and select one child per household to be the survey subject. A parent or guardian knowledgeable about the child completes the survey via web- and paper-based instruments, and results are weighted to be representative.74 However, given the address-based sample, children experiencing homelessness are unlikely to be included in the survey, suggesting that the survey likely underestimates the prevalence of extreme adversity. Moreover, the surveys are available in only English and Spanish, which excludes children from non-Spanish-speaking, linguistically isolated households. These represent significant limitations of the NSCH and other large population-based surveys.
To increase the size of the analytic sample in order to produce more reliable estimates, CAP followed NSCH guidance to combine data across the most recent three years of surveys: 2016, 2017, and 2018.75 CAP adjusted individual-year survey weights in order to reflect an average annual population and then restricted the dataset to children younger than age 4 with complete data on all ACEs items, resulting in a final analytic sample of 17,999 observations representing 14.6 million young children nationwide. The rate of incomplete ACEs data was low; about 5 percent of children in this age group had missing ACEs data and were excluded from the final sample.
CAP used parents’ responses to the following questions to derive the findings: 76
- To the best of your knowledge, has this child EVER experienced any of the following? (Yes/No)
- Parent or guardian divorced or separated
- Parent or guardian died
- Parent or guardian served time in jail
- Saw or heard parents or adults slap, hit, kick, punch one another in the home
- Was a victim of violence or witnessed violence in his or her neighborhood
- Lived with anyone who was mentally ill, suicidal, or severely depressed
- Lived with anyone who had a problem with alcohol or drugs
- Treated or judged unfairly because of his or her race or ethnic group
- SINCE THIS CHILD WAS BORN, how often has it been very hard to get by on your family’s income—hard to cover the basics like food or housing? (Very Often, Somewhat Often, Rarely, Never). Answers of “very often” and “somewhat often” were coded as having experienced this ACE.
CAP calculated the relative confidence interval for each estimate by dividing the absolute 95 percent confidence interval by the estimate and multiplying by 100. Consistent with previous research from Child Trends, if the relative confidence interval for a given estimate—for example, the percentage of Asian American children with two or more ACEs—is more than 120 percent, CAP deemed the estimate unreliable and suggests interpreting with caution.77
CAP tested for statistical significance between state and national estimates by comparing the 95 percent confidence intervals. If the confidence intervals did not overlap, the differences are marked as significant.78 The same approach was used for determining differences between racial and ethnic groups and age-related differences. To determine racial and ethnic disparities, CAP used non-Hispanic white children as the reference group, whereas to determine age-related differences, CAP used infants younger than age 1 as the reference group.
When sample sizes for racial and ethnic groups were too small to yield reliable estimates for ACEs prevalence, CAP combined several categories into “non-Hispanic other.” Included in the non-Hispanic other category are children reported as Native Hawaiian or Pacific Islander (n=23, or 1.4 percent of the total number of children in this category); American Indian and Alaska Native (n=75, or 4.5 percent of the total number of children in this category); two or more races (n=1,401, or 84.7 percent of the total number of children in this category); or another race not already listed (n=156, or 9.4 percent of the total number of children in this category). These group estimates are available upon request. Although the NSCH precludes further analysis of multiracial individuals, previous research has found that the majority of individuals identifying as two or more races have Native American ancestry.79
An important limitation of the NSCH, especially in the context of child development, is its cross-sectional nature. Because the same children are not surveyed year to year, the authors are unable to draw any conclusions about how exposure to adversity changes over individual children’s life span. Instead, findings about how ACEs differ across age is based on unique samples of children in each age group.
Additional analyses
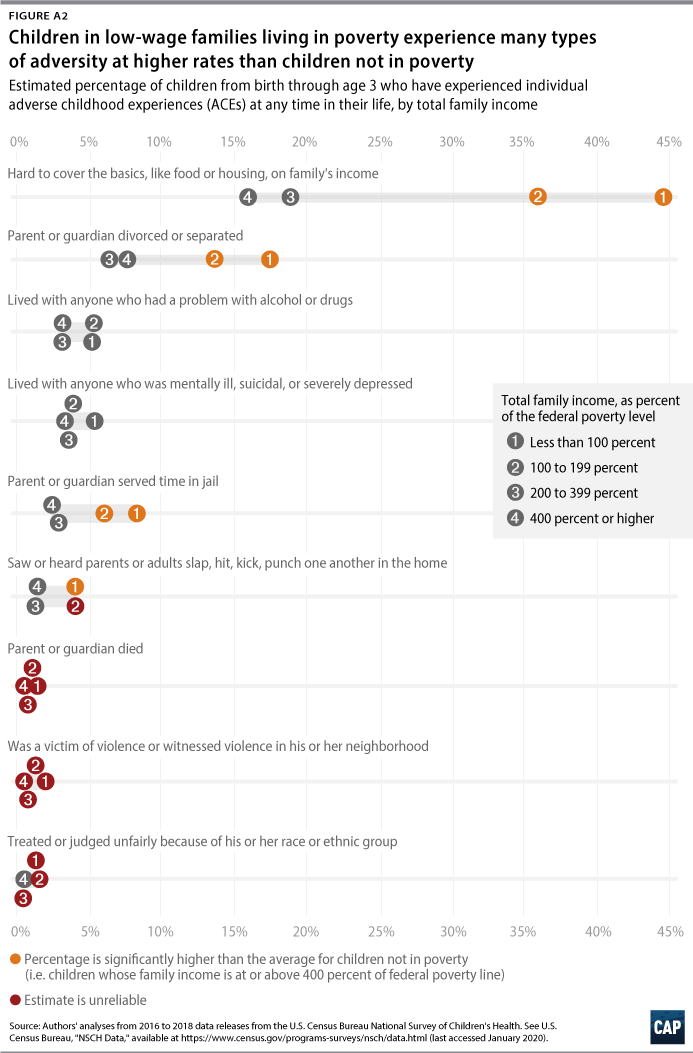
Additional analyses show that children across the socioeconomic spectrum are exposed to adversity. (see Appendix Figure 1 and Appendix Figure 2)
To find the latest CAP resources on the coronavirus, visit our coronavirus resource page.