Click here to view the full-size version of the interactive in this report.
Introduction and summary
In August 2016, Connecticut parents learned that the state’s child care assistance program, Care 4 Kids, would stop enrolling most children due to insufficient funding.1 In a state where families can expect to pay more than $20,000 a year to send two children to a child care center, this news was devastating to many parents.2 One such parent was Annunziata Zito, a mother with two children ages 8 and 3. Without assistance from Care 4 Kids, she thought she might have to quit her job, leaving her family living in poverty.3
Connecticut was an early adopter of a new federal requirement to extend eligibility for child care assistance to a full year.4 The change was based on evidence from child development experts that shows providing consistent child care is important for young children.5 Continuous access to high-quality child care promotes strong relationships and positive interactions with early educators, which in turn supports skills such as vocabulary, early literacy skills, and healthy behaviors. But with children staying in the program longer and no new federal or state resources, Connecticut could no longer enroll new children. In the year that followed, the number of children receiving child care assistance through Care 4 Kids was cut by more than 40 percent. This particularly affected parents with infants, who could not enroll their babies when they returned to work. After Care 4 Kids stopped enrolling new children, the number of infants and toddlers in the program dropped from 8,200 to 4,400.6
Connecticut’s experience was a bellwether for the country. For decades, federal and state lawmakers underfunded child care assistance, resulting in dwindling enrollment levels and fewer quality options for parents as the value of their child care voucher eroded over time. Congress took action in 2014 to improve quality, requiring minimum safety protections, such as background checks for child care providers, and extending eligibility periods for child care assistance.7 But without additional funding, these improvements exacerbated declines in enrollment for child care assistance. By 2016, child care assistance plummeted across the country and the federal Child Care and Development Block Grant (CCDBG) program served the fewest children in its 18-year history.8
While Connecticut is one of the wealthiest states in the nation, it is also one of the most unequal.9 The bottom 20 percent of households earn less than $30,000 annually, while the top 20 percent of households have incomes in excess of $140,000.10 One in 5 young children lives in a low-income working family, with at least one parent employed most of the year.11 This means in Connecticut, families who most need child care in order to work cannot afford the high price of tuition without child care assistance.
In addition to affecting child care assistance, Care 4 Kids’ enrollment freeze affected parent’s child care options. Connecticut’s child care supply dwindled as 250 family child care homes and 140 child care centers shut their doors.12 In wealthier towns where families could afford private tuition prices, the child care market remained strong. But in poorer cities and towns such as Hartford, New Haven, and New Britain—where average incomes hover below $40,000 a year—child care programs were hit hard when parents could no longer afford them. In fact, 10 months after Care 4 Kids stopped accepting new enrollees, more than half of the decline in enrollment accrued in the 10 lowest-income municipalities.13
Care 4 Kids ultimately reopened enrollment in November 2017, and enrollment levels have since then risen.14 A recent increase in federal funding gave Care 4 Kids a $14 million additional boost,15 allowing the program to increase enrollment, raise assistance levels for families, and expand the supply of infant and toddler child care.16
Connecticut’s experience underscores the importance of public funding in supporting access to child care programs and sustaining the supply of child care in low-income areas. In fact, Connecticut invests more per child in its child care subsidy system than most other states.17 But without a more robust public investment in child care, parents cannot afford the cost of care and supply declines in areas with higher concentrations of low-income households.
For too long, federal and state governments have underfunded child care, leaving many communities without licensed child care options. And such options are a necessity for working families: Two-thirds of U.S. children who have not started school have all parents in the workforce. At the same time, the cost of child care is out of reach for the average family; in most areas of the country, it exceeds the costs of rent or in-state college tuition.18
While the principles of supply and demand would usually suggest that child care providers would gravitate to underserved areas, the fact that providing child care costs more than most families can afford results in an imbalance between supply and demand. This market failure is especially problematic, because it affects children in their formative years when their experiences are shaping the cognitive, language, and socio-emotional skills that influence future learning.
Recent polling suggests that most parents struggle to find child care. Among parents with a child under age 5, 83 percent reported that finding quality, affordable child care was a serious problem in their area. Parents feel the impact of limited child care options in the work place: the same poll found that child care issues negatively affected the careers of three-quarters of parents with young children.
To better understand the U.S. supply of licensed child care and national trends in families’ proximity to child care, the Center for American Progress analyzed the geographic locations of licensed child care facilities, including centers and family child care homes. This analysis assesses trends in proximity to child care as one component of a child’s ability to attend a high-quality early childhood program. To describe this geographic proximity, in 2016, CAP introduced a working definition of child care deserts—areas with an insufficient supply of licensed child care.19 In 2017, CAP analyzed data from 22 states, covering two-thirds of the U.S. population.20 This year, the analysis includes data from all 50 states and Washington, D.C., and finds that more than half of Americans—51 percent—live in neighborhoods classified as child care deserts.
Other key findings from this year’s report include:
- Families in rural areas face the greatest challenges in finding licensed child care, with 3 in 5 rural communities lacking adequate child care supply. High-income suburban neighborhoods are the least likely to experience child care shortages.
- Hispanic/Latino families disproportionately reside in child care deserts, with nearly 60 percent of their population living in areas with an undersupply of licensed child care.
- Child care deserts have, on average, maternal labor force participation rates that are 3 percentage points lower than those of communities where there is adequate child care supply.
- The prevalence of child care deserts varies from state to state, from fewer than 23 percent of Maine neighborhoods to more than 75 percent of Utah neighborhoods.
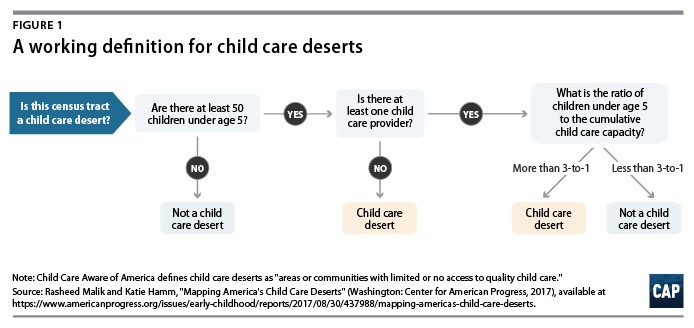
This report uses the definition of child care deserts established in CAP’s 2017 report, “Mapping America’s Child Care Deserts,” such that a ratio of more than three young children for every licensed child care slot constitutes a child care desert. (see Figure 1 for additional detail) This definition is derived from U.S. Census Bureau findings showing that approximately one-third of young children are regularly in the care of someone who is not a relative.21 When the number of licensed child care slots is insufficient to reach at least one-third of young children under age 5, the likelihood that parents face difficulty finding child care increases. This could affect employment decisions or force families to turn to unlicensed options.
Many parents face the difficult task of finding child care that is convenient to work or home and does not break the bank. This study builds on researchers’ understanding of why the child care search often involves stress, waiting lists, high costs, and compromises. Understanding the supply of child care is only one piece of solving the U.S. child care crisis: In addition to geographic proximity, families consider cost, availability of child care assistance, operating schedule, facilities, and preferred characteristics of the potential caregiver. Yet, while geographic proximity is not the only factor in the accessibility of licensed child care, the absence of licensed child care in a community often means it is not an accessible option for parents. Shedding light on who lives near licensed child care can serve as a catalyst for a broader conversation about making affordable, quality child care a reality for all families.
After detailing the CAP analysis, this report considers how to address the issue of child care supply without compromising children’s safety, as well as how to address the child care needs of underserved groups such as families with infants and toddlers, families with people with disabilities, immigrant families, and parents that work nontraditional hours. The report also recommends policy solutions to address access to high-quality child care options. Unfortunately, conversations about child care supply sometimes question whether safety regulations should be relaxed to lower costs and encourage more providers to enter the market. This would be a misguided approach to solving the problem; no parent wants their child in a facility that has not undergone proper inspection or in a setting with too many children present for adults to safely provide care. Instead, policymakers and advocates should identify ways to build the supply of high-quality options from which parents can choose by expanding public investment in child care and intentionally building supply across all settings.
Analyzing America’s child care deserts
For this report, the Center for American Progress collected and analyzed data on the location and capacity of licensed or registered child care providers in every state and Washington, D.C. These data were synthesized with estimates of the population, family income, and labor force participation rates in every one of the country’s 73,057 census tracts. This original and comprehensive analysis of child care supply at the census tract level finds that 51 percent of Americans live in child care deserts. This term, as used by CAP, is adapted from terminology applied to the problem of “food deserts.”22 In this report, the authors describe child care deserts as areas with little or no licensed child care capacity. As shown in Figure 2, the proportion of residents living in child care deserts ranges from 22 percent in Maine to 77 percent in Utah. For more information on the authors’ methodology, see the Appendix.
This analysis only includes licensed family child care homes and centers in the United States, though a significant number of families rely on relatives, friends, or neighbors for child care. This type of child care—known as family, friend, and neighbor care (FFN); kith and kin care; or license-exempt care— is a common child care arrangement for many families. (see text box for more information)23 This study excludes FFN providers, because states typically do not keep records of license-exempt providers. And while understanding usage rates for FFN care provides a more complete picture of the child care landscape, it is not necessarily informative of overall child care supply. For example, a grandmother may decide to care for her granddaughter until she enters school, but that arrangement does not represent a slot that is available to other children in the community.
Click here to view the full-size version of this interactive.
Overall, rural areas have the highest concentration of child care deserts
For this report, each of the more than 73,000 census tracts in the country is assigned to one of three urbanicity types—rural, suburban, or urban—based on a measure of household density, which considers the number of occupied households per square mile.24 Using this measure, about 20 percent of the population is categorized as rural; 25 percent lives in high-density urban neighborhoods; and 55 percent resides in suburban, medium-density neighborhoods. This estimate of the rural population is in line with other estimates of the proportion of Americans living in rural areas, including that of the U.S. Census Bureau.25
Overall, rural census tracts are the most likely to be classified as child care deserts, with 59 percent of rural communities meeting that definition. This study is careful to include licensed family child care providers, as home-based child care is the most common child care setting in rural areas.26 Nonetheless, there is a vast undersupply of child care infrastructure across most of rural America. While rural communities may have several home-based child care providers, many family child care homes are only licensed to serve between six and 12 children, which may not be able to meet demand.27
Urban neighborhoods are also more likely to be child care deserts than not, with 56 percent of urban census tracts showing child care supply gaps. While suburban neighborhoods are relatively less likely to be child care deserts, about 44 percent of suburban families find themselves in neighborhoods with too few child care options, and waiting lists can still be common, particularly for infant and toddler care.28
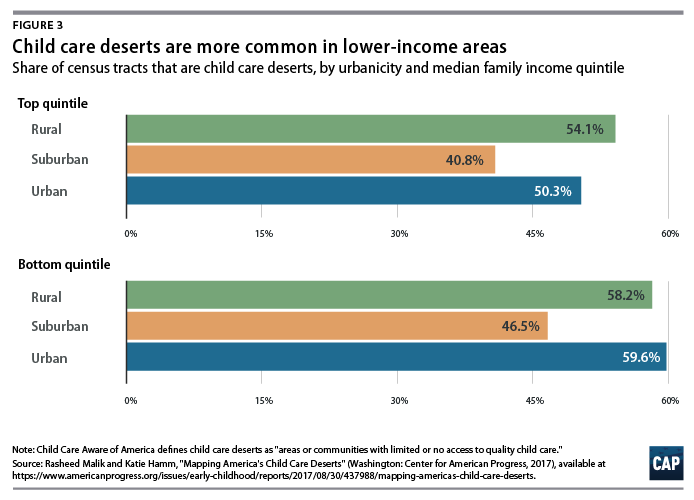
When these urbanicity categories are further broken down by the typical family income in each census tract, a more nuanced picture emerges. (see Figure 3) The authors assigned each neighborhood to a family income quintile, ranking all census tracts in the state by median family income. The 20 percent of neighborhoods in which the median family income is highest fall into the top income quintile, the next 20 percent are assigned to the next quintile, and so on, with the lowest median income neighborhoods in the bottom income quintile.
With this additional information, urban areas in the bottom income quintile have roughly the same rate of child care deserts as the average rural area. As shown in Figure 3, neighborhoods in the top income quintile are less likely to be undersupplied within each geographic category, and suburban areas in the top income quintile are the least likely of all neighborhood-income types to be a child care desert. Considering the public underinvestment in child care financing, it should not be surprising that the licensed child care market gravitates to neighborhoods with more families who can afford to pay full tuition.
Certain characteristics of cities make it challenging to accurately capture child care availability in urban areas. This study compares the population of young children who live in a given census tract with the availability of licensed child care slots in that area. However, census tracts in urban areas tend to be very small due to high population density, making it likely that many urban families use child care providers that are located outside of the census tract in which they live. These factors could lead to an over- or underestimation of the demand for child care in a given urban area. Because cities are so densely populated, an analysis specifically looking at urban child care supply must be hyperlocalized to fully understand the dynamics of the child care market in these communities.
Nonetheless, several conditions in urban areas likely contribute to a high concentration of child care deserts in low-income areas. While cities may have a high concentration of child care centers, employment opportunities, and public transportation, these amenities tend to be concentrated in wealthier areas and not necessarily available to all residents.29 Child care is also costlier to provide in cities, because labor and real estate are more expensive. Home-based providers in urban areas often operate in apartment buildings or other high-density housing locations, which have less space and can accommodate fewer children than providers in rural or suburban communities. These providers must also address the concerns of their neighbors and landlords, who may not support a child care business in a shared residential setting.30 Urban child care providers may also face barriers to finding space where children can be safely cared for. For example, children under the age of 2 typically must be cared for on the ground floor of a building so that they can be safely evacuated in case of an emergency.31
Hispanic/Latino populations disproportionately live in child care deserts
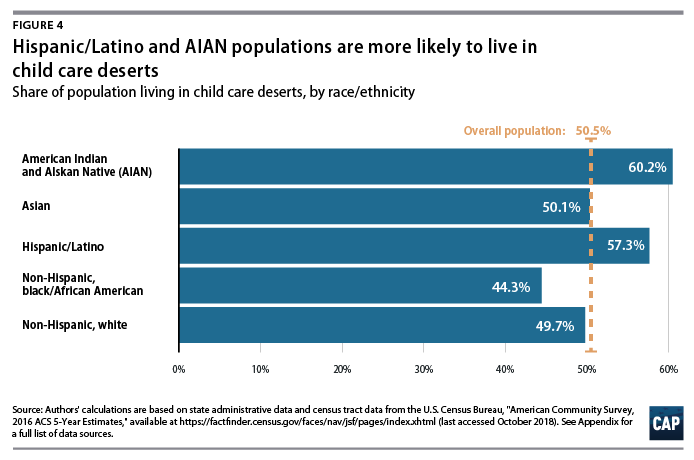
This study analyzes the proportion of each neighborhood’s population residing in child care deserts, using the race and ethnicity categories as defined by the U.S. Census Bureau. (see Appendix for full details) The data show that the Hispanic/Latino population is highly overrepresented in child care deserts,32 as seen in Figure 4. It should be noted, however, that proximity to licensed child care does not necessarily mean that people have access to these programs. Each racial and ethnic group may face systemic barriers such as high prices, low wages, and historic disenfranchisement and discrimination.33
Hispanics/Latinos are the fastest-growing racial/ethnic group in the United States; one-quarter of all children in the United States are Hispanic/Latino, and they are projected to constitute one-third of the child population by 2050.34 Yet these families are more likely to live in areas with fewer child care options. All approaches to increasing the supply of child care in America will need to remedy the fact that child care seems to be consistently harder to find in communities with a high concentration of Hispanics/Latinos.
Child care researchers and advocates have long speculated that Hispanic/Latino families may have a cultural preference for informal or relative care over formal or nonrelative child care arrangements. The National Research Center on Hispanic Children and Families investigated many of these assumptions and found that the perceptions of Hispanic/Latino parents, whether they are immigrants or native-born, on different types of child care arrangements are generally similar to those of black and white non-Hispanic parents. In an analysis of the 2012 National Survey of Early Care and Education, these researchers found that, for children ages 3 through 5, there was very little difference between Hispanic/Latino children’s participation in early care and education and the participation of children from other racial/ethnic groups.35
However, among children younger than age 3 in low-income families, researchers did find significantly lower rates of participation in early care and education programs among immigrant Hispanic/Latino households when compared with native-born Hispanic/Latino households.36 To that point, this study finds that children who live in areas with the highest share of foreign-born parents are about 13 percent more likely to live in a child care desert than those in who live in areas with the lowest share of foreign-born parents. Findings from this research also suggest that Hispanic/Latino immigrant and native-born households are more likely than non-Hispanic/Latino households to need care during nonstandard hours and to have a grandparent or teen living in the household.37 This suggests that Hispanic/Latino families have uniquely diverse child care needs and preferences. For this reason, this study cannot conclude that higher rates of child care deserts in Hispanic/Latino communities are entirely attributable to lack of demand.
This study also finds that American Indian and Alaska Native (AIAN) families are likely to live in child care deserts. However, the census estimates used in this study only count people who identify as AIAN alone, which may undercount the total AIAN population. It should be noted that the AIAN alone population is much more likely to live on rural tribal lands than the 40 percent of AIAN people who identify as multiracial.38 Because tribal lands are generally exempt from state licensing jurisdiction, these findings should be interpreted with caution. Many tribes do, in fact, license child care independent of state licensing systems, per the regulatory guidance offered by the U.S. Department of Health and Human Services.39 The authors did not solicit information on the location of child care programs licensed by tribes; thus, this study is unlikely to capture the full child care market in those areas.
The poverty rate for AIAN families with children under age 5 is estimated to be 74 percent higher than the rate for the rest of the U.S. population, underscoring the deep need for high-quality child care in these communities.40 The child care needs of AIAN families are understudied, and additional research could provide information on how best to support these families and provide resources to tribal governments so that they can meet demand.
Child care deserts are correlated with lower rates of maternal labor force participation
Improving access to consistent and affordable high-quality early care and education accomplishes two important objectives: It promotes healthy child development, and it allows parents to work or to re-enter the labor force after taking leave. This applies to women in particular, as mothers traditionally spend more time caregiving than fathers do and are more likely to leave the labor force to care for children.41
In addition to looking at racial and ethnic patterns of child care availability, this study examines the relationship between child care deserts and parental labor force participation. The labor force participation rate measures the number of people who are currently employed or actively looking for a job as a proportion of all civilian, noninstitutionalized adults.42
 This report finds that child care deserts are associated with labor force participation rates for mothers with young children that are roughly 3 percentage points lower than the participation rates in neighborhoods with adequate child care supply. This difference is not observed in men’s labor force participation rates. It is more pronounced among mothers with children under age 6—in other words, mothers for whom quality child care could potentially affect their ability to work.43 When the sample is restricted to census tracts in the bottom quintile for family income, this labor force participation gap becomes even larger. Among these low-income areas, child care deserts are associated with maternal labor force participation rates that are nearly 5 percentage points lower than those in nondeserts.
This report finds that child care deserts are associated with labor force participation rates for mothers with young children that are roughly 3 percentage points lower than the participation rates in neighborhoods with adequate child care supply. This difference is not observed in men’s labor force participation rates. It is more pronounced among mothers with children under age 6—in other words, mothers for whom quality child care could potentially affect their ability to work.43 When the sample is restricted to census tracts in the bottom quintile for family income, this labor force participation gap becomes even larger. Among these low-income areas, child care deserts are associated with maternal labor force participation rates that are nearly 5 percentage points lower than those in nondeserts.
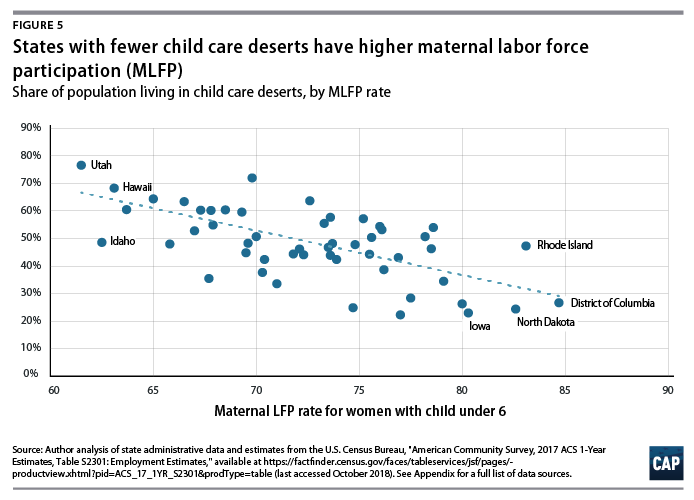
By comparing every state’s maternal labor force participation rate with the prevalence of child care deserts, this report finds a strong correlation between the two measures. As the maternal labor force participation rate increases, the share of the population in that state living in a child care desert declines. (see Figure 5) Using a simple linear regression, these data show that a 1 percentage-point increase in maternal labor force participation is associated with a 1.6 percentage-point decline in the share of the population living in a child care desert.
What about FFN care?
Child care that occurs in a home that is not licensed is called family, friend, and neighbor (FFN) care.44 Most of these providers are exempt from state licensing, because they are caring for a relative or because the number of children in the provider’s care falls below the state’s licensing threshold. According to analysis by the National Women’s Law Center, approximately 24 percent of children under age 6 are in home-based child care with a relative, and an additional 13 percent are in home-based care with a nonrelative.45 The latter group, however, includes children in licensed family child care—thus, it is difficult to ascertain a precise estimate of children in FFN care. However, a sizeable portion of families with young children use this type of child care arrangement, and children with disabilities and infants are more likely to be in FFN care.46
Parents select FFN care for a variety of reasons. Many families who use this type of child care prefer that their child stay with a trusted relative or friend or seek a setting that provides culturally relevant care, while others may feel that FFN care provides a more nurturing environment that mirrors the child’s home environment. For others, FFN best meets their child care needs. As more parents have nonstandard work hours and require child care in the evenings or on weekends, FFN providers are far more likely to provide care when licensed child care programs are closed.47 In fact, parents who use FFN care cite availability and reliability as top reasons for choosing their provider.48
For some families, FFN care is the only option they can afford. Most FFN providers are unpaid,49 and low-income families are more likely to rely on FFN care than licensed care.50 For families living in child care deserts without many licensed child care options, FFN providers may be the only available option.
Research suggests that there are differences in children’s experiences across child care settings. On average, children in FFN care engage in fewer learning activities designed to promote cognitive skills that prepare children for school.51 For example, 4-year-olds in FFN care watch two hours of TV per day on average, while 4-year-olds in formal care settings watch an average of fewer than seven minutes per day.52 Ninety-three percent of formal caregivers report reading activities every day, compared with 68 percent of FFN caregivers.53 These differences have been directly tied to gaps in children’s school readiness. In fact, by age 5, children who attended classroom-based preschool have stronger reading and math skills than those who attended informal FFN settings.54
Whether families turn to informal care by choice or out of necessity, FFN care is filling a critical gap in America’s underfunded child care market. It is imperative that all families have access to the child care provider of their choice, and if they prefer FFN care, FFN providers must be equipped with the supports necessary to ensure that the care they provide is safe and enriching.55
Addressing child care supply without compromising safety
It is not surprising that child care deserts are pervasive across the country: There is a clear disparity between the revenue that providers need to operate a child care program and how much parents can afford to pay. Operating a safe and high-quality child care center—one that pays its teachers a living wage and trains them to be effective educators; has small adult-to-child ratios to promote safety, language development, and social and emotional skills; and invests in age-appropriate materials and classroom spaces—is expensive.56 Child care providers usually close their doors, because they simply cannot afford to operate on tuition payments alone, leading to an undersupply of child care across the country.57
Efforts to bolster child care supply must focus on growing financially sustainable child care programs and protecting children’s safety. Operating a child care center or family child care home is costly, but some elements that drive costs are necessary to protect children’s safety and put them on the path to healthy development. Policies that attempt to cut costs by rolling back safety protections, reducing teacher wages, or increasing classrooms sizes will ultimately backfire by undercutting quality and reducing the effectiveness of early childhood investments.
Promoting safety protections is also popular with voters. A recent poll found that 92 percent of voters support standards to improve quality and safety in child care.58 As policymakers consider strategies to address child care deserts, there are several key components of safe, quality child care that must be bolstered to promote child well-being—not sacrificed to reduce costs.
Basic safety protections
When parents take their children to a licensed child care center or home, they expect that the program will meet some basic standards that protect young children from harm. Other industries that provide services to the public—such as restaurants, nail salons, and even pet groomers—receive regular inspections and certifications to ensure they are safe and following best practices. In 2014, Congress passed legislation to bring child care to the same standard as other industries.59 Federal policies now require first-aid and CPR trainings for staff, comprehensive background checks for adults who interact with children, and annual monitoring visits. These evidence-based safety protections help ensure that teachers are vetted and able to care for children and that physical care environments are safe for young children.60
Yet, while the federal government requires states to set minimum standards, states have flexibility in determining standards beyond these and in implementing health and safety requirements, leading to some differences in state standards for child care providers. When baseline safety measures are not met or are improperly implemented, the consequences can be fatal.61 As states consider building child care infrastructure, maintaining these safety protections must be an equal priority.
Teacher wages, supports, and trainings
In addition to health and safety, a well-paid and effective early childhood workforce is a critical component of building child care supply. The most important marker of a quality child care program is responsive and nurturing interaction between adults and children. Yet, a chronically underfunded child care system has resulted in extremely low pay for early childhood educators, with the median child care worker earning just $10.72 per hour. As a result, turnover is high in the child care industry.62 Paying teachers a living wage is a key component of child care quality, as an educator’s ability to be attentive and responsive to the children in her care is closely tied to their own economic security.63 More than half of U.S. child care workers participate in a public assistance program, and early educators report significant levels of stress related to earning poverty-level wages.64 Pay for early childhood educators is another priority for American voters, with 9 in 10 Americans supporting proposals to ensure that people working in child care earn a living wage, according to a recent poll.65 With persistently low wages already threatening child care quality, pay for early educators must be increased—not further reduced—to build up and strengthen the supply of quality child care options across the country.
Teacher-child ratios and group size limits
In addition to pay, the number of children in an adult’s care contributes to program quality and can either promote or undermine positive interactions. Adult-child ratios dictate how many children can be safely cared for by a single adult, and group size limits cap the number of children that can be cared for in a classroom or home. For example, the National Association for the Education of Young Children, which sets national accreditation standards for the highest-quality child care programs, recommends a ratio of 1 adult for every 4 infants, with a maximum class or group size of eight babies with two adults per class or group.66 These standards are in place for good reason: Young children require constant supervision and attention, and an adult simply cannot provide responsive attention when there are too many children in their care. Group size limits are also important in determining when a home-based provider must become licensed. States determine the enrollment threshold for licensing, which requires a provider to register with the state and abide by certain health and safety regulations.
Research shows that lower teacher-child ratios and group size limits are key to ensuring a child’s safety and promoting classroom quality; in fact, teachers in settings with lower ratios tend to be less stressed, provide children with more individualized attention, and engage in more dialogue with children.67
Together, these key components of safe and quality child care are paramount for protecting child safety, as well as for ensuring that parents have high-quality child care options from which to choose. If safety standards are relaxed, parents will be left with fewer child care options they can trust, further exacerbating the issues of child care deserts. Rather than cutting corners to cut costs, policymakers must strive to support providers, so in order to offer care that is both safe and affordable.
The effects of child care deserts for specific populations
This analysis primarily considers the relationship between child care deserts and demographic characteristics such as urbanicity, race and ethnicity, and employment trends. But as mentioned above, geographic proximity is only one factor in determining whether a child has access to licensed child care. And close proximity may not promote access to child care for certain populations who have difficulty finding child care programs that meet their families’ needs. For example, families with infants and toddlers; parents with disabilities and parents of children with disabilities; immigrant families; and parents working nonstandard hours have all historically faced limited options for licensed child care, as described in detail below.
Infants and toddlers
Most parents discover that child care is harder to find when their children are infants than when they are preschoolers. When child care supply is examined by age group, licensed options are much scarcer for the youngest children.
In a recent report, the Center for American Progress examined nine states that provided child care supply data for specific age groups and found that child care slots were more than three times scarcer for infants and toddlers than they were for preschoolers.68 Using the child care deserts threshold of at least one licensed child care slot for every three children, more than 95 percent of the counties in that analysis would be considered infant-toddler child care deserts.69 Consistent with the findings of this report, infant-toddler child care shortages were found to be worse in rural and lower-income areas.
Infant and toddler child care is scarcer than care for other age groups largely because it is more expensive to provide. Infants and toddlers require more supervision and interaction with adults, making smaller staff ratios essential. In addition, child care subsidy rates cover an even smaller portion of the cost of providing quality care for infants and toddlers than they do for preschoolers.70 As a result, providers struggle to care for young children at a price that families can afford.
The near-universal shortage of licensed child care for infants and toddlers has negative consequences for working parents. When parents are unable to access care for their young children, many are forced to make career sacrifices. A recent survey found that 77 percent of parents of young children stated that they or someone in their family experienced negative impacts to their career because of child care considerations.71 Even if parents stay in the workforce, they often must weave together a patchwork of care arrangements that lacks the quality assurances of licensed care. In addition, child care teachers who work with infants and toddlers face a so-called wage penalty, earning an average of $2 less per hour than teachers serving older children, even when controlling for education level.72
Families that include people with disabilities
In 2016, more than 1.1 million children under age 6—or about 5 percent of the United States’ early childhood population—received services related to their disability.73 In addition, about 2.5 percent of parents of young children have a disability that affects their ability to work.74 For families who have either a child or parent with a disability, access to quality child care involves much more than just proximity to a center with available slots; it means finding a program willing to enroll and work closely with families to provide appropriate care. Although several federal laws support the right of children and parents with disabilities to access early childhood educational programs and child care, families often struggle to find and keep services.75
The Individuals with Disabilities Education Act guarantees educational opportunities for eligible children with disabilities from birth through age 21, including preschool special education and early intervention services for infants and toddlers.76 Although these programs help children access critical developmental and educational services, they were not designed to meet working parents’ child care needs. For example, most states’ preschool special education programs—which enroll more than 450,000 preschoolers—operate on an academic calendar.77 This means that working parents of children who enroll in these preschool programs must find other child care arrangements after school and during the summer months. For children younger than age 3, early intervention services often consist of home visits to deliver services. These families may need to find full-time child care in addition to early intervention programs.
The Americans with Disabilities Act (ADA) and Section 504 of the Rehabilitation Act prohibit discrimination based on disability.78 The ADA stipulates that, with a few exceptions, child care programs cannot exclude children with disabilities unless including them requires a “fundamental alteration of the program.”79 Moreover, programs must make “reasonable modifications” to integrate individuals with disabilities. But because these terms are open to interpretation—and because programs often operate on razor-thin margins that make paying for modifications difficult—families frequently find themselves excluded. Although all parents struggling to find affordable, quality child care face barriers to service, these barriers are exacerbated for families that include people with disabilities. They include:
- Care that is too expensive, especially since families of children with special needs face more economic difficulties80
- Program policies requiring children to be toilet trained and use the bathroom independently81
- Program policies prohibiting providers from administering medications82
- Staffing shortages and high adult-child ratios that make it difficult to provide individualized attention83
- Suspension or expulsion of children with challenging behaviors84
- Facilities that do not accommodate the physical needs of some children or parents with disabilities, such as no automatic doors, which can affect individuals with certain mobility-related disabilities85
- Lack of support from providers, often due to lack of training86
The availability of child care—particularly for parents of children with disabilities and parents with disabilities—has a profound effect on parents’ employment as well as their mental and emotional well-being.87 Without the support that comes from reliable, quality child care, parents can suffer from the acute stress of arranging care for their children, care that is often of an unreliable or inconsistent quality. This comes on top of the numerous other barriers that individuals with disabilities and their families may face. Unfortunately, individuals with disabilities and their families too often find themselves excluded from many child care settings.
Children in immigrant families and dual-language learners
Like their peers with native-born parents, most children in immigrant families have all available parents in the workforce.88 However, they are much less likely to enroll in early care and education programs.89 Indeed, in a nationally representative sample of low-income families with children younger than age 5, less than half of children of immigrants had a regular child care arrangement—a significantly lower rate than that seen among children of U.S.-born parents. The difference in program enrollment was even more stark for children younger than 3. Only 40 percent of infants and toddlers in immigrant families were enrolled in regular child care, compared with 52 percent of their peers with U.S.-born parents.90 Analysis of CAP’s child care deserts data finds that children who live in areas where more foreign-born parents live are about 13 percent more likely to live in a child care desert than those in areas with few or no foreign-born parents.
Although conventional wisdom has attributed lower participation rates to immigrant parents’ preference for familial care, recent studies suggest that the child care attitudes of immigrant and U.S.-born parents are more similar than they are different. For example, one study found that although foreign-born parents were less likely to use child care overall, those who did enroll their children in nonparental child care were as likely to choose center-based care as their U.S.-born counterparts. Moreover, immigrant and U.S.-born parents’ responses were similar when asked to rate the importance of different program characteristics, such as a nurturing environment, preparing children to learn in school, teaching social skills, affordability, and flexibility.91
Several studies show that immigrant and limited English proficient parents want the same opportunities for their children as U.S.-born parents but are simply less able to access them. Barriers to participation include:92
- Insufficient program outreach
- Program oversubscription
- Inconvenient locations, hours, and schedules
- Inadequate translation and interpretation services
- Distrust of government institutions
Addressing these barriers and expanding access to child care for children in immigrant and dual-language families is critical, as these groups represent a growing share of the future workforce. Moreover, research shows that they may benefit more from high-quality early care and education than children from U.S.-born families, as the care helps offset challenges related to growing up with parents who have low English proficiency.93
Parents who work nontraditional hours
Millions of parents, particularly low-wage workers, have nontraditional and unpredictable working hours and require child care during nights or on weekends. In fact, 58 percent, or 2.76 million, of low-income children under the age of 6 have a parent who works at least some hours between 6:00 p.m. and 8:00 a.m.94 These families face difficulty finding child care that aligns with their work schedules, as most child care providers operate during the regular workday: Just 8 percent of center-based and about a third of home-based providers offer care during the evenings, overnight, or on weekends.95 As such, most parents who work nontraditional hours turn to care from family, friends, and neighbors, or piece together multiple care arrangements.96 In areas that already face a shortage of child care options, finding providers that operate during nontraditional hours is an added barrier for working families.
The additional expenses providers face when offering care during nontraditional hours present a barrier to increasing supply of this type of child care. Many shift workers have irregular work schedules, making demand for care during nontraditional hours inconsistent. For example, a provider might have five children who need after-hours care one night, but just one child who needs it the next. This irregularity presents challenges for providers in terms of staffing and other planning needs. Furthermore, finding early educators who are able and willing to work through the night and on weekends is difficult and expensive. As a result, research finds that child care centers that offer more flexible schedules have teachers with lower levels of education and professional learning.97 Overnight care also requires providers to be equipped with additional resources such as beds, as well as to implement additional trainings for staff that might not otherwise be necessary.98
As policymakers grapple with finding approaches that can make quality, affordable child care a reality, considering the unique needs of a diverse group of families is necessary. While the data in this analysis show that families across the United States are struggling to find affordable child care, it is important to take into account the specific barriers faced by certain populations, as these barriers can have a significant impact on their ability to access child care programs that meet their needs.
Policy recommendations
Federal and state policymakers can take steps to address child care deserts and expand access to affordable, quality child care. These steps include: improving data collection, increasing public investments in child care and early education, raising child care payment rates, and making child care infrastructure investments in all child care settings.
Improve data collection
Analyzing supply and demand data will help policymakers determine the policy solutions needed to address the child care supply gap. States should prioritize data collection that allows policymakers, advocates, and researchers to accurately assesses the number of children, by age group, that licensed child care providers serve. Accurate data on the local child care market can help advocates and provider networks design nuanced interventions to ensure they are meeting the needs of families. For example, a thorough data analysis can determine if a state has a need for increased supply serving infants and toddlers, child care subsidy-eligible children, children with disabilities, parents with nonstandard hours, children of immigrants, or English-language learners.
Increase public investments in child care and early education
Without financing to support the provision of high-quality child care, supply will continue to be an issue for families who cannot afford high tuition rates. Recently, Congress increased funding for the Child Care and Development Block Grant (CCDBG), which states are using to increase the number of families served through the child care subsidy system.99 While this increase is already improving access to quality child care, a much larger investment is needed to fully fund high-quality child care.
In 2017, Sen. Patty Murray (D-WA) and Rep. Bobby Scott (D-VA) introduced the Child Care for Working Families Act, which would make affordable, quality child care a reality for all families by limiting parents’ child care payments to 7 percent of their annual income, or about $45 a week for the average family.100 This legislation would also improve child care quality and increase pay for early educators. Importantly, the bill focuses on children birth to age 5 with an emphasis on child care for infants and toddlers, who have been largely left out as states and cities expand preschool.101
Raise child care payment rates
A key way to increase access to high-quality programs is to increase child care subsidy reimbursement rates based on the real costs of operating a program. Currently child care subsidy payments cover only a fraction of market rates—or the amount that child care programs charge parents paying out of pocket. The recent increase in CCDBG funding is helping many states increase payments to child care providers. Unfortunately, this rate still reflects the current realities of the child care market, where early educators are underpaid, and programs struggle to cover the costs of operation.
Conducting a cost-of-quality study can help states determine the actual costs to operate a high-quality early childhood program, including sufficient teacher compensation. States can then set reimbursement rates based on this study, including variations by quality, ensuring that programs are not disincentivized from serving child care subsidy-eligible children and that programs serving primarily low-income children are able to generate sufficient revenue to operate at a high-quality level. Such studies should also consider additional costs associated with serving infants and toddlers, children with disabilities, and families who need child care during nonstandard hours.
Make child care infrastructure investments in all child care settings
Efforts to invest in infrastructure tend to enjoy bipartisan support. After all, building bridges, roads, and transit systems is critical to the nation’s economy. Equally important to America’s infrastructure is ensuring that families have access to high-quality, affordable child care. This includes updating child care and early education facilities—including Head Start facilities—and licensed family child care homes. The National Children’s Facilities Network estimates that the cost of upgrading child care facilities, including Head Start facilities, to current professional quality standards is $10 billion.102 This includes updating building space to address health and safety issues, repair structures, upgrade utilities, and ensure classrooms are developmentally appropriate for children. Federal funds for facilities upgrades should be distributed via the Community Development Financial Institutions Fund, which is designated by the U.S. Department of the Treasury.103
Investing in child care infrastructure also means supporting licensing and monitoring systems, as well as taking steps to support the early childhood workforce. Importantly, infrastructure investments must be paired with long-term financing strategies to ensure that programs can afford to operate.
Conclusion
The American child care market, in its current form, depends on public investment to help meet demand, as a purely market-driven approach to providing quality child care for the nation’s children leaves out most middle-class and low-income families. Fortunately, funding for the child care subsidy system has been increased for the next fiscal year, which gives states the opportunity to raise their reimbursement rates, thereby granting families much-needed relief from the high prices associated with quality child care.104
In Connecticut, state administrators plan on using the increase in their child care development funds to support licensed capacity for infants and toddlers.105 The state will be raising its reimbursement rates for infants and toddlers in child care centers from the fourth percentile of the market rate to the 70th percentile, which means it will now cover $17,000 per year, per child in child care costs for qualified families with an infant in center-based care.106
Connecticut hopes to incentivize child care providers to accept infants and toddlers by offering a $500 one-time payment for each child they enroll through the state’s child care subsidy system. For the young children they enroll who don’t qualify for child care subsidies, the providers will still receive a $100 bonus. Additionally, the state is contracting directly with family child care providers to help create 500 new infant and toddler spots in family child care homes.107
Connecticut’s example shows that child care supply is directly linked to the level of public investment that policymakers deem appropriate. For many years, the United States has lagged behind other advanced nations when it comes to child care investment.108 Consequently, the labor force participation rate of parents with young children, especially mothers, has remained flat even as the economy has improved. Supporting working families through more substantial public investment is a commonsense, evidence-backed approach to building a supportive and growth-minded society and economy.
About the authors
Rasheed Malik is a senior policy analyst for Early Childhood Policy at the Center for American Progress.
Katie Hamm is the vice president of Early Childhood Policy at the Center.
Leila Schochet is the research and advocacy manager for Early Childhood Policy at the Center.
Cristina Novoa is a policy analyst for Early Childhood Policy at the Center.
Simon Workman is the associate director of Early Childhood Policy at the Center.
Steven Jessen-Howard is a research assistant for Early Childhood Policy at the Center.
Acknowledgements
The authors would like to thank Chaley Kirkpatrick for her invaluable research assistance. This project is only now possible because state child care licensing agencies and nonprofit child care referral agencies have begun publishing their data on the internet and/or providing child care data available upon request. The authors are thankful to these public and nonprofit sector agencies and employees for this public service.
Appendix: Methodology, data sources, and limitations
The methodology in this analysis is largely based on the methods employed in CAP’s 2017 report, “Mapping America’s Child Care Deserts.”109 This section includes previously published notes on the methodology from that report and is updated to reflect the fact that the 2018 analysis includes all 50 states, which required new methods for securing data from additional states.
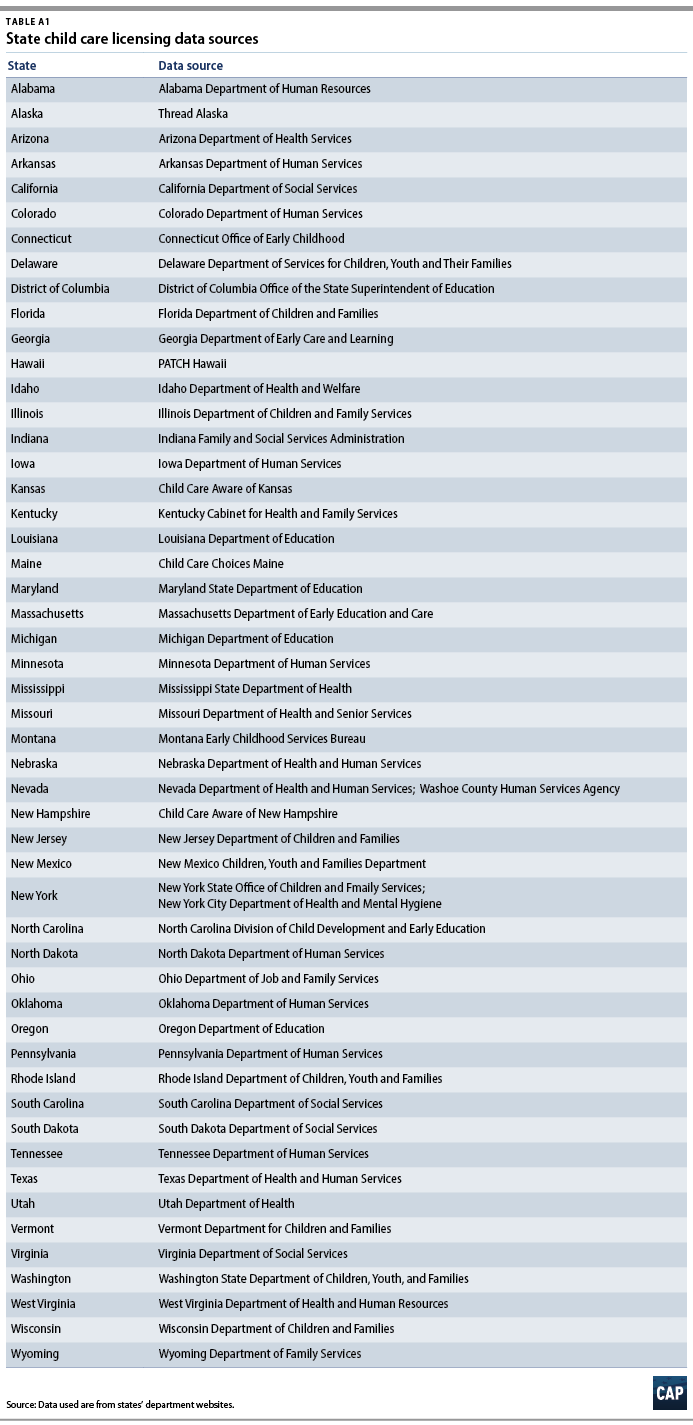
The authors collected 2018 data on the location and maximum capacity of all licensed or registered child care providers in all 50 states, plus Washington, D.C. (see Table A1 for data sources) This includes child care centers; family child care providers; Head Start and Early Head Start providers; and pre-K classes. In approximately 24 states, the authors downloaded publicly available tables of state licensing databases on a government website, usually within a department of human services or child and family services. For another 20 states, the authors directly contacted the departments responsible for child care licensing in that state and made successful public requests for the child care data. Finally, in seven states that did not respond to requests for child care data, the authors used a web crawler to gather and copy data from public child care search sites. This technique is commonly referred to as web scraping or web harvesting and was only done in these cases of last resort.110
Once this information was collected, the authors cleaned the data to remove any duplicates and child care providers whose licenses had expired or been suspended. All summer camps or after-school care providers were excluded—except those child care providers who also offered after-school capacity—because this study looks at the supply of child care for children from birth to age 5 who are not yet enrolled in elementary school. In these cases, the number of school-age children was deducted from the overall capacity of the child care location. Except in cases of Head Start providers, licensed child care centers were top-coded to a maximum capacity of 200 children. In total, this analysis included 234,540 child care locations, with a combined total capacity of approximately 9,200,000 child care slots.
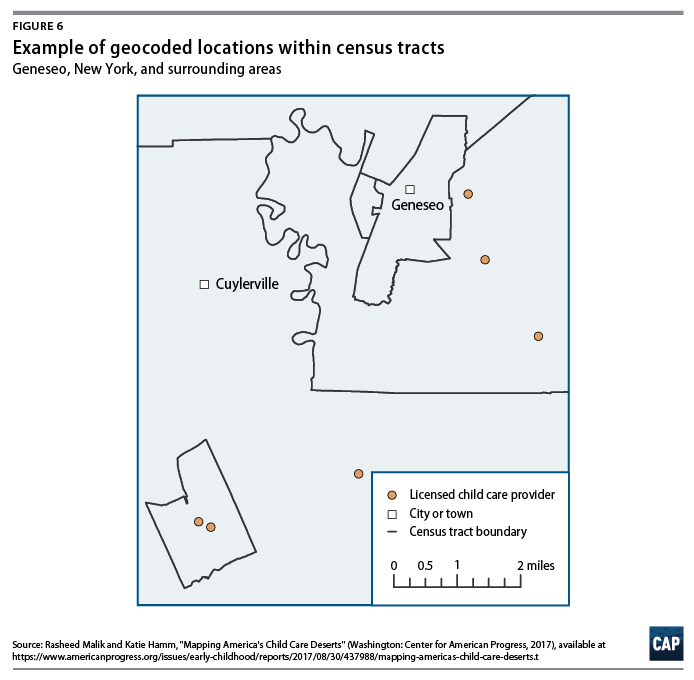
Next, the authors used geocoding software to convert the location data from street addresses to precise latitude and longitude coordinates. This resulted in a data set with a count of child care locations and a sum of capacity for each census tract. In total, the analysis included 73,057 census tracts.
Methodology
CAP collected data on the location and licensed capacity of nearly 235,000 licensed or registered child care providers from every state plus Washington, D.C. The authors included all child care centers; family child care providers; Head Start providers; and public and private preschools in these states in order to get a full picture of the supply of licensed child care options available to nearby communities.
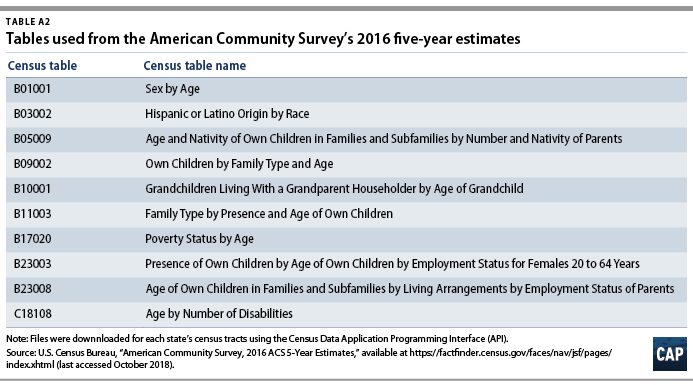
Each child care provider was geocoded based on the physical address provided on their license, giving the authors a precise latitude and longitude for every provider. In cases where the precise address was not available, the authors used the ZIP code to approximate the address. CAP then grouped providers by census tract and added up the total licensed capacity of the locations in each tract. This information was merged with a variety of census estimates on population demographics, population density, family income, poverty, and maternal labor force participation, among other variables. A list of data sources and census variables can be found in Table A2.
Using this original data set, the authors applied the child care deserts definition to thousands of census tracts, a geographic unit sometimes used by city planners to approximate neighborhoods.111 Census tracts generally have a population size of between 1,200 and 8,000 people, with most tracts housing around 4,000 people. These geographic units usually cover a contiguous area, and their boundaries commonly follow identifiable features, such as rivers, city boundaries, or county lines.112
This data set of child care locations and capacity by census tract was then merged with variables from 11 census tables, all of which are listed in Table A2. Not all variables listed were used in the analysis, but they are presented here nonetheless. Once these variables were merged with the counts of child care locations and capacity, the authors generated a binary variable to identify child care deserts using CAP’s working definition for child care deserts, as shown in Figure 1.
One of the goals of this research was to analyze whether rural, suburban, or urban areas have differing levels of child care supply. Since, to a certain extent, these categories are a subjective evaluation, this question poses a formidable challenge. Inspired by research by economist Jed Kolko, this study uses household density—that is, the number of occupied households per square mile—to categorize each census tract as rural, suburban, or urban.113 The results were analyzed by mapping the resulting data set in ArcGIS.
This study has some limitations, largely related to the assumptions that are used to define child care deserts. As with any complex analysis, the underlying assumptions will not suit every scenario. This analysis, and the working definition of a child care desert, assumes that families prefer child care that is closer to their home. While this may be true for many families, some child care arrangements work better when they are closer to a parent’s employer or school. Besides location, there are other factors that figure into a child care decision that this analysis cannot fully model. For instance, child care is often driven by hours of need or a child’s age. While, in the aggregate, this study may accurately estimate the overall undersupply of licensed child care, the problem is likely worse for those seeking child care during nonstandard hours, including weekends and evenings.114
Some of the analysis’ limitations result from incomplete data. Some state databases do not include complete data, requiring some imputation on the part of the authors. California, Oregon, and Washington state do not release the full addresses of family child care providers, though they do provide ZIP codes. These family child care providers were geocoded to the center of the associated ZIP code, and then placed into the corresponding census tract for that location. In Pennsylvania, Alabama, and South Dakota, some portion of child care providers did not report their full licensed capacity. In these cases, the authors imputed the maximum licensed capacity for that type of child care provider. Finally, Mississippi and New Jersey do not license family child care homes, so these providers were not included in this analysis for those two states.