Several states are beginning to relax their stay-at-home orders without specifying or meeting key thresholds for safely reopening their economies. Such arbitrary loosening, unmoored from evidence and conditions on the ground, risks a second uncontrollable wave of coronavirus infections. This result would necessitate a second round of lockdowns comparable to the first, in effect wasting the progress that has been made and deepening the economic downturn.
There are at least three key thresholds for states to meet before they can substantially relax their stay-at-home orders:
- Transmission is controllable because there is a low level of incidence—the rate of occurrence of new cases.
- Testing capacity is adequate to detect outbreaks and identify and isolate positive cases as well as their contacts.
- A high percentage of contacts can be traced because the state has a minimum number of contact tracers and minimum adoption of instantaneous contact tracing technology.
This column specifies the first two thresholds using South Korea as a model, as it is the only country—other than small island nations—that has successfully controlled coronavirus transmission without a lockdown. South Korea provides the only evidence in the real world of conditions under which coronavirus can be controlled.
After specifying evidence-based incidence and testing thresholds for each state, this analysis finds that no state currently meets both thresholds; only eight states meet an incidence threshold; and only Rhode Island meets the testing threshold.
Evidence-based incidence thresholds
Some experts have recommended that states can safely reopen if there is a sustained decline in positive cases over 14 days. But the epidemic curve is asymmetric: The downward slope from the peak is much more gradual than was the upward slope to the peak, resembling more of a plateau. This means that widespread, uncontrollable transmission will likely remain even 14 days after the peak.
For this reason, the absolute level of incidence—not just the trend—is critically important. Simply put, incidence needs to be low enough that a strategy of testing, contact tracing, and isolation can suppress any coronavirus outbreak. When there is widespread transmission, this strategy is not feasible. Moreover, if widespread transmission remains, the public will not have confidence in engaging with the economy—regardless of whether it is legally allowed.
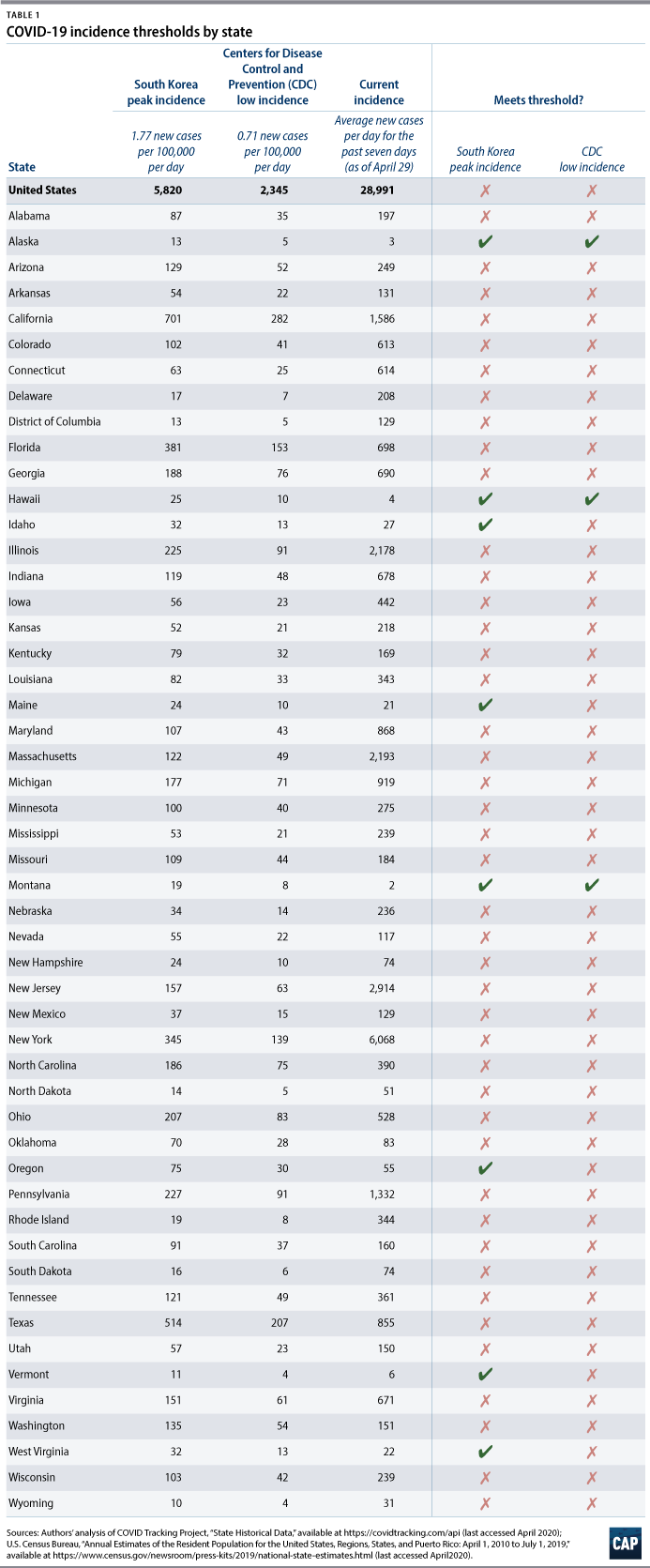
In South Korea, the incidence was 1.77 new cases per 100,000 people per day at its peak—a rate that was controllable. Applied to the U.S. population, this rate is equivalent to about 5,800 new coronavirus cases per day in the United States. Currently, the United States is averaging about 28,900 new cases per day—over the past seven days.* Table 1 presents this incidence threshold for each state based on state populations. Only eight states—Alaska, Hawaii, Idaho, Maine, Montana, Oregon, Vermont, and West Virginia—currently meet this threshold.
An alternative incidence threshold is based on what the Centers for Disease Control and Prevention (CDC) considers to be low incidence. The CDC defines low incidence as 10 or fewer new cases per 100,000 people over a period of 14 days. This rate is equivalent to 0.71 new cases per 100,000 people per day, or about 2,300 new cases per day in the United States. Table 1 presents this incidence threshold for each state based on state populations. Only Alaska, Hawaii, and Montana currently meet this threshold.
Some regions in a state may have much lower incidence than others; conversely, some regions may have severe coronavirus outbreaks, even if the statewide incidence is low. Therefore, states may decide to apply these evidence-based thresholds, measured in new cases per 100,000 people, to regions.
Evidence-based testing thresholds
South Korea had enough testing to achieve a positive coronavirus rate of 2 percent. According to epidemiologists, a low positive rate is an indication that testing is widespread enough to catch nearly all of the infections in the population. In comparison, as of mid-April, the United States had a positive rate of 18.7 percent.
States need enough testing capacity to achieve a positive rate of 2 percent, even if cases rise to a moderate level due to an outbreak after stay-at-home orders end. Although others have recommended state testing levels by deriving actual cases from deaths, model projections of deaths six weeks from now are highly variable, with wide uncertainty, and deaths are vastly underreported. To avoid the need to estimate actual cases, this analysis assumes that the CDC’s moderate incidence case level reflects the actual number of cases at a positive rate of 2 percent. When the positive rate is 2 percent, indicating sufficient testing coverage, states can be confident that the number of confirmed cases is very close to the actual, true number of cases.
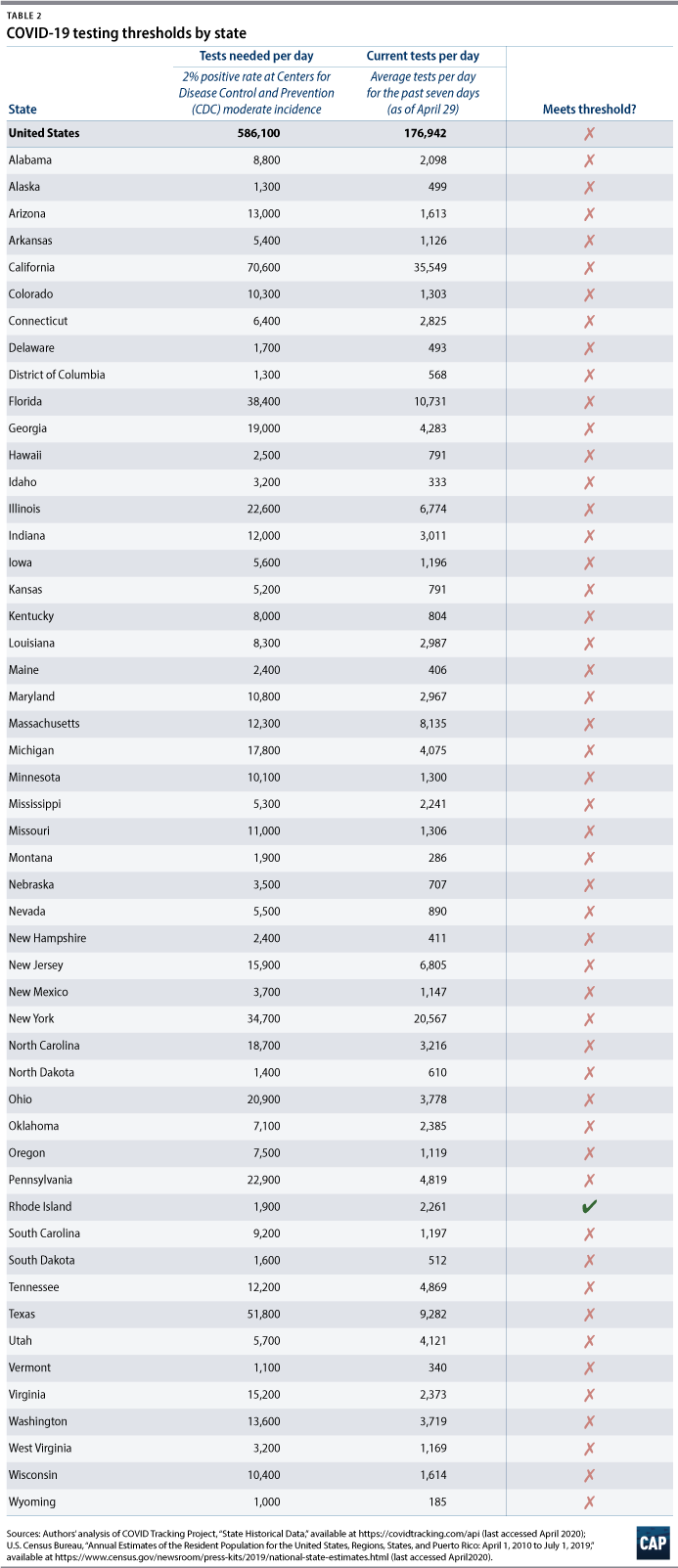
The CDC defines moderate incidence as up to 50 new cases per 100,000 people over a period of 14 days. At this incidence, the United States would need approximately 586,100 tests per day—or 179 tests per 100,000 people per day—to achieve a current positive rate of 2 percent. Currently, the United States is averaging about 176,900 tests per day—over the past seven days. Table 2 presents this testing threshold for each state based on state populations. Only Rhode Island currently meets this threshold.
Conclusion
Based on evidence-based thresholds for incidence and testing, no state is ready to substantially relax its stay-at-home order. In addition, states would also need to meet metrics for capacity to conduct robust contact tracing.
We know what works. And the purpose of stay-at-home orders in the first place was to suppress coronavirus transmission to low levels and buy time to ramp up testing and contact tracing. States must not lose sight of this purpose and overall strategy. If they do, the stay-at-home orders will need to be repeated, wreaking havoc on Americans’ lives and the economy.
Topher Spiro is the vice president of Health Policy and a senior fellow for Economic Policy at the Center for American Progress. Emily Gee is the health economist of Health Policy at the Center.
* Authors’ note: The Center for American Progress calculated this figure and other COVID-19 statistics using state data from the COVID Tracking Project that were current as of 4:00 p.m. on April 29.
To find the latest CAP resources on the coronavirus, visit our coronavirus resource page.