States have the duty and public health authority to protect the health and safety of their residents. To do so effectively, states rely on federal support in the form of guidance, technical support, and funding, which typically comprises only about 3 percent of all federal spending on health. In the best of times, this funding level leaves states with a significant gap in resources to address needs such as data system modernization, public health workforce expansion and diversification, disease monitoring and public health laboratory functioning, injury prevention, and climate and environmental health. But in the absence of even baseline federal support—and in the face of increasing health threats such as the ongoing measles outbreak in Texas—states are in a truly challenging position. Recognizing this, it is more important than ever for state policymakers to find opportunities to reinforce critical public health protections, mitigate some of the negative impacts of the Trump administration’s policies on peoples’ lives and health, and safeguard the health and safety of their residents. State leaders must seize opportunities to protect public health authorities, invest in public health infrastructure, uphold scientific integrity and counter dangerous rumors and falsehoods, and mitigate environmental health risks.
1. Protect public health authorities
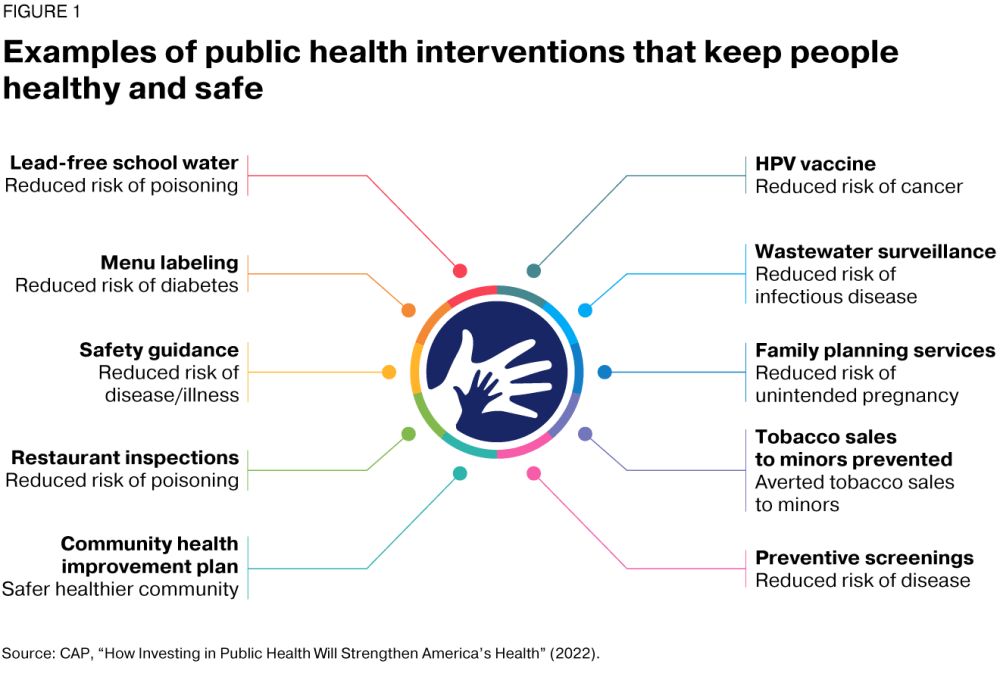
The authority to implement public health measures is a fundamental legal tool that allows state policymakers to mitigate disease and protect and preserve the lives and health of the American people. States use this authority to promote health during disease outbreaks and public health crises and to address ongoing adverse conditions that harm communities’ health and well-being, such as exposure to pollution and unsafe environments. This authority allows state leaders to create and implement policies and plans and to enforce regulatory actions, such as inspecting food establishments for safe practices, monitoring wastewater for signs of infectious diseases circulating within communities, and engaging in other ways the public health system works to protect individuals and communities and to promote health and well-being. (see Figure 1)
![]()
The current H5 bird flu outbreak among poultry and dairy cattle, while not yet a public health emergency, is a pressing example of an emerging threat to which public health officials must be ready to quickly and effectively respond. State and local health officials need organizational independence and decision-making authority in order to move swiftly should bird flu adapt to enable human-to-human transmission.
Yet since the COVID-19 pandemic began in 2020, many state legislatures have attacked and chipped away at public health authorities by taking steps to delay, limit, or eliminate certain public health interventions. These include measures to limit core authorities such as isolation and quarantine guidelines, identification and investigation of disease outbreaks, and development of state vaccination policies. These limitations hinder responses to public health emergencies. In fact, states with more limited emergency public health authorities experienced more COVID-19 deaths during 2021–2022. State policymakers should work closely with health officials to restore these authorities at both the state and local levels to respond effectively to public health emergencies.
State policymakers should work closely with health officials to restore these authorities at both the state and local levels to respond effectively to public health emergencies.
Vaccination is an essential tool to reduce disease and improve public health
Read more
2. Invest in core public health infrastructure
Despite tremendous public health achievements in preventing diseases and extending life expectancy, unstable federal funding that creates a “boom-bust cycle of support” limits states’ capacities to address core public health needs. This affects issues ranging from chronic disease prevention to pandemic response. Alarmingly, more than half of local health department funding comes from federal sources. Complicating federal funding instability—and in spite of growing public health threats—the Trump administration has signaled its commitment to making indiscriminate cuts to the public health infrastructure that enables public health agencies to protect and promote health. Cuts to National Institutes of Health funding would erode research on treating and preventing diseases and would affect jobs and economies in every state, as would plans to slash staff and programs at the Centers for Disease Control and Prevention (CDC), the primary federal agency that funds state and local public health programs.
Read more
States supplement federal funding with state and local resources such as taxes, fees, and third-party reimbursements. California, for example, provided in its 2024–2025 budget an annual investment of nearly $300 million to its state and local public health departments that has supported cancer prevention and treatment, promotion of locally grown fresh fruits and vegetables within nutrition benefit programs, mental health services, and medication-assisted treatment for opioid users. And Kentucky’s biennium budget for fiscal years 2025 and 2026 includes a $1 million increase in fiscal year 2026 for local health department staffing and operations.
Particularly at a moment when federal funding is at risk, dedicating state investments to public health infrastructure, as well as enhancing those investments, would improve health and ensure resilience against emerging threats. For instance, in the event that federal public health data modernization efforts stall, investments in state-level data systems will be particularly useful to facilitate tracking and sharing of emerging disease data across state borders.
State funding for public health ranges anywhere from $7 to $423 per person annually. Although state leaders will be challenged to supplement federal funding shortfalls, at a minimum they can prioritize sustained funding: At least 37 states and Washington, D.C., either maintained or increased their public health funding in FY 2023. The Indiana legislature, for example, increased public health funding by 1,500 percent in 2023, with a requirement that counties provide a 20 percent match.
3. Uphold scientific integrity and counter rumors and falsehoods
When federal actions undermine proven public health practices and further erode public trust, states can serve as champions for scientific integrity, engaging experts and prioritizing evidence-based information to inform policy and public health decision-making and protect the health of Americans. State health officers and surgeons general should be important expert voices selected for their positions based on commitment to supporting evidence-based decision-making. They should be empowered to issue clarifying guidance when federal communications mislead or conflict with evidence-based practices. State health officials should be empowered to educate the public on specific health interventions using trusted information sources, without undue restrictions, to address or get ahead of misinformation.
When federal actions undermine proven public health practices and further erode public trust, states can serve as champions for scientific integrity, engaging experts and prioritizing evidence-based information to inform policy and public health decision-making and protect the health of Americans.
Public health departments must be able to provide timely, accurate, clear, and practical information during health emergencies to encourage appropriate action and build public trust. State leaders must invest in public health departments to advance these goals through expanded communications capacities, enhanced crisis communication skills, and more effective health communication. With additional resources, public health departments can improve health communications through tailored messaging for different audiences, partnerships with trusted community leaders, and monitoring for misinformation.
State and local health officials must also prioritize evidence-based policies that protect the health and safety of residents, which sometimes may require disregarding federal recommendations. For example, water systems should continue to fluoridate public drinking water, regardless of Trump administration biases, given the long-standing evidence that fluoride at recommended levels is safe and effective at preventing tooth decay, the most common childhood chronic disease in the United States.
4. Mitigate environmental health risks
Environmental toxins and extreme weather conditions pose significant risks to public health and safety. In fact, leading researchers describe climate change as this century’s greatest threat to public health globally and have linked climate change to increases in infectious disease, chronic illness, and mental health. Yet on his second day in office, Secretary of Health and Human Services Robert F. Kennedy Jr. terminated funding for climate change and health programs at the National Institutes of Health. The Trump administration has imposed mass terminations at the U.S. Environmental Protection Agency (EPA) and cut programs aimed at reducing climate hazards and protecting the most burdened communities from environmental contaminants in the air and water. The administration has canceled funding to secure clean air and water, rolled back environmental protections; paused drafts in the regulatory review process, including those that set standards for reducing PFAS, or forever chemicals, and eliminating lead pipes that carry drinking water; and plans to reverse pollution standards for smog, soot, and air toxins, along with emission requirements for power plants, vehicles, coal waste, and oil refineries.
In the absence of continued federal action and the cancellation of critical protections, states must lead on environmental protections and climate policies. For example, states can accelerate the clean energy transition in key sectors by adopting clean electricity standards, holding polluting electric power companies accountable, streamlining siting and permitting processes for clean energy projects, and supporting community solar. States should also pursue efforts that protect individuals and communities from the consequences of climate change. Enacting state-level occupational heat standards, especially given the Trump administration’s regulatory freeze that stalls the proposed federal heat standard, will safeguard workers from extreme heat. Protections against eviction and utility shutoffs, rebates for efficient heat-pump air conditioning, and programs to help families pay their electricity bills could also help those at higher risk of death and illness from extreme heat stay safe during extreme heat events.
Finally, states should continue efforts to regulate environmental toxins in air and water that are linked to asthma, cancer, heart disease, reproductive health harms, child development delays, and other health conditions. Only 12 states have standards regulating PFAS in drinking water. More states should adopt PFAS standards that at a minimum align with the recently enacted and reversed federal standard. States can set statewide goals and continue to provide education and outreach on lead service line replacement. They can also enact policies to improve indoor air quality in public spaces and develop plans to reduce soot pollution in their counties to align with the EPA standard adopted in 2024.
Conclusion
States carry an outsize responsibility and constitutional duty to protect public health. Without cohesive, evidence-driven federal leadership, states must implement actions that defend and amplify proven public health interventions, strengthen public health systems, and mitigate risks to health.